

Four-dimensional velocity mapping of the hepatic and splanchnic vasculature with radial sampling at 3 tesla: a feasibility study in portal hypertension
- PMID: 21751287
- PMCID: PMC3417100
- DOI: 10.1002/jmri.22712
Four-dimensional velocity mapping of the hepatic and splanchnic vasculature with radial sampling at 3 tesla: a feasibility study in portal hypertension
Abstract
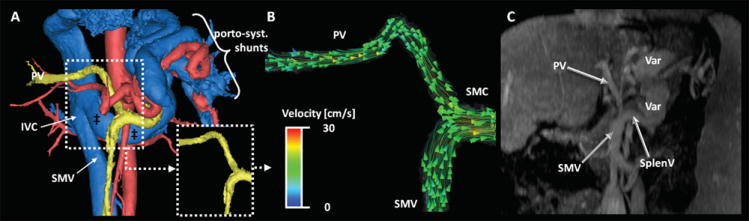
Purpose: To demonstrate the feasibility of PC-VIPR (Phase Contrast Vastly undersampled Imaging with Projection Reconstruction) for the depiction and hemodynamic analysis of hepatic and splanchnic vessels in patients with portal hypertension.
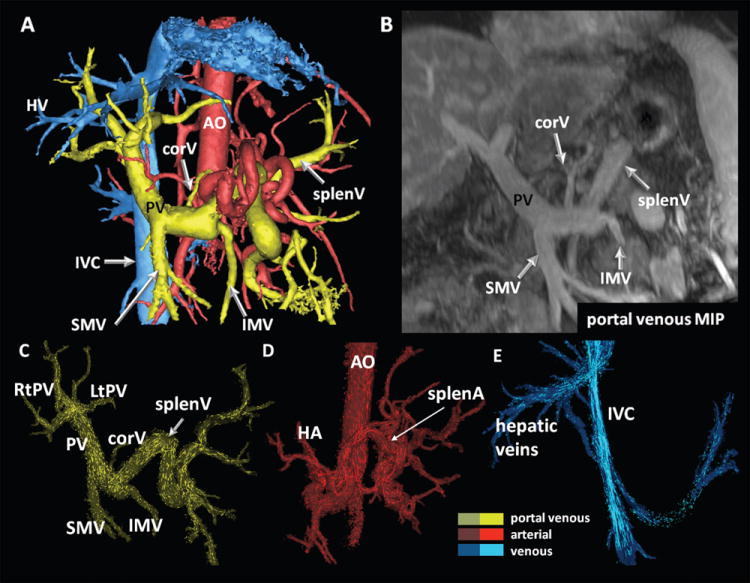
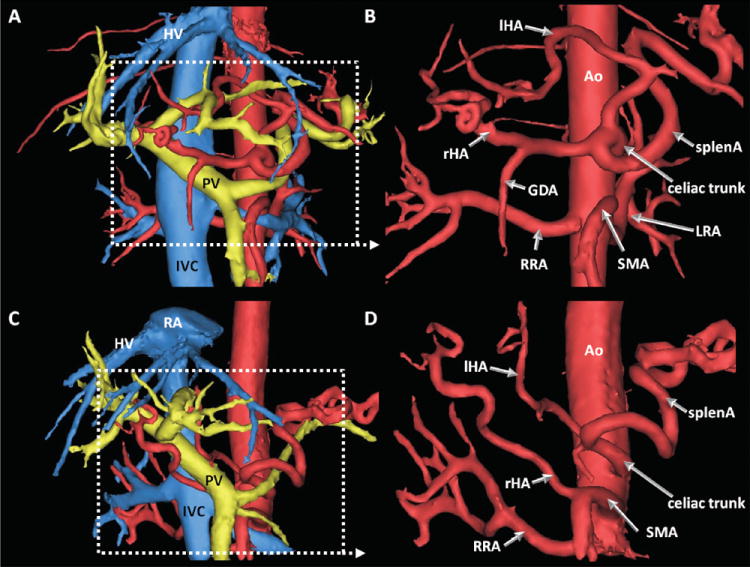
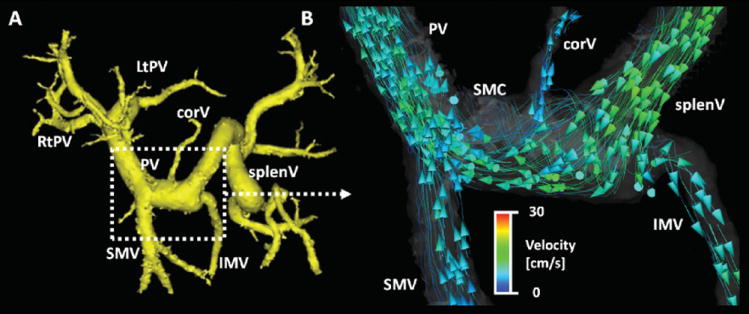
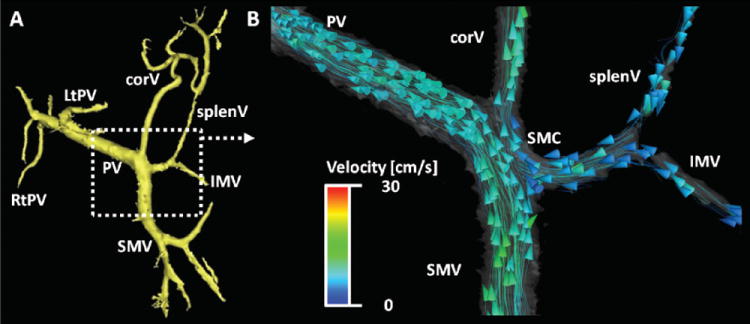
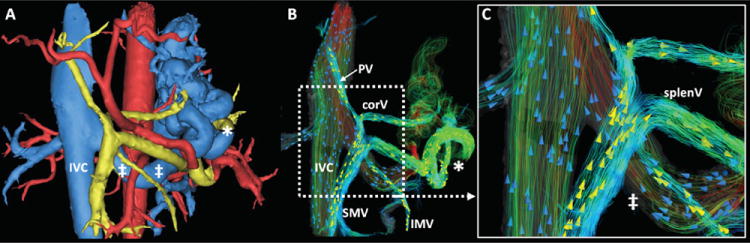
Materials and methods: Twenty-four cirrhotic patients (55.9 ± 10.4 years) were scanned using 5-point PC-VIPR for high spatial resolution imaging with large volume coverage at 3 Tesla (T) using a 32-channel body coil. Vessel segmentation and hemodynamic visualization included color-coded three-dimensional (3D) streamlines and particle traces. Segmentation quality was compared with contrast-enhanced multi-phase liver imaging. Flow pattern analysis was performed in consensus of three readers. The MELD score was calculated to estimate disease severity and was correlated to image quality.
Results: Good to excellent visualization quality was achieved in 23/24 cases. All arterial vessels and 144/168 vessels of the portal venous (PV) circulation were unambiguously identified. No correlation with the MELD score was found. Eight of 148 vessels of the PV circulation demonstrated reverse (hepatofugal) flow. Hepatofugal flow in small tributaries to PV flow were present in three cases despite hepatopetal flow in the PV.
Conclusion: This feasibility study demonstrates the feasibility of PC-VIPR for simultaneous morphological and hemodynamic assessment of the hepatic and splanchnic vasculature in cirrhosis and portal hypertension. Future studies with quantitative analyses are warranted.
Copyright © 2011 Wiley-Liss, Inc.
Figures
References
-
- McCullough AJ. Pathophysiology of nonalcoholic steatohepatitis. J Clin Gastroenterol. 2006;40(Suppl 1):S17–29. - PubMed
-
- Ratziu V, Bonyhay L, Di Martino V, et al. Survival, liver failure, and hepatocellular carcinoma in obesity-related cryptogenic cirrhosis. Hepatology. 2002;35(6):1485–1493. - PubMed
-
- Moreau R, Lebrec D. Molecular Mechanisms of Systemic Vasodilatation and Hyperdynamic Circulatory State of Cirrhosis. In: Sanyal AJ, Shah VH, editors. Portal Hypertension: Pathobiology, Evaluation, and Treatment, Clinical Gastroenterology. Totowa, NJ: Humana Press; 2005.
-
- Applegate GR, Thaete FL, Meyers SP, et al. Blood flow in the portal vein: velocity quantitation with phase-contrast MR angiography. Radiology. 1993;187(1):253–256. - PubMed
-
- Burkart DJ, Johnson CD, Morton MJ, Wolf RL, Ehman RL. Volumetric flow rates in the portal venous system: measurement with cine phase-contrast MR imaging. AJR Am J Roentgenol. 1993;160(5):1113–1118. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
