

Top-down quantitative proteomics identified phosphorylation of cardiac troponin I as a candidate biomarker for chronic heart failure
- PMID: 21751783
- PMCID: PMC3170873
- DOI: 10.1021/pr200258m
Top-down quantitative proteomics identified phosphorylation of cardiac troponin I as a candidate biomarker for chronic heart failure
Abstract
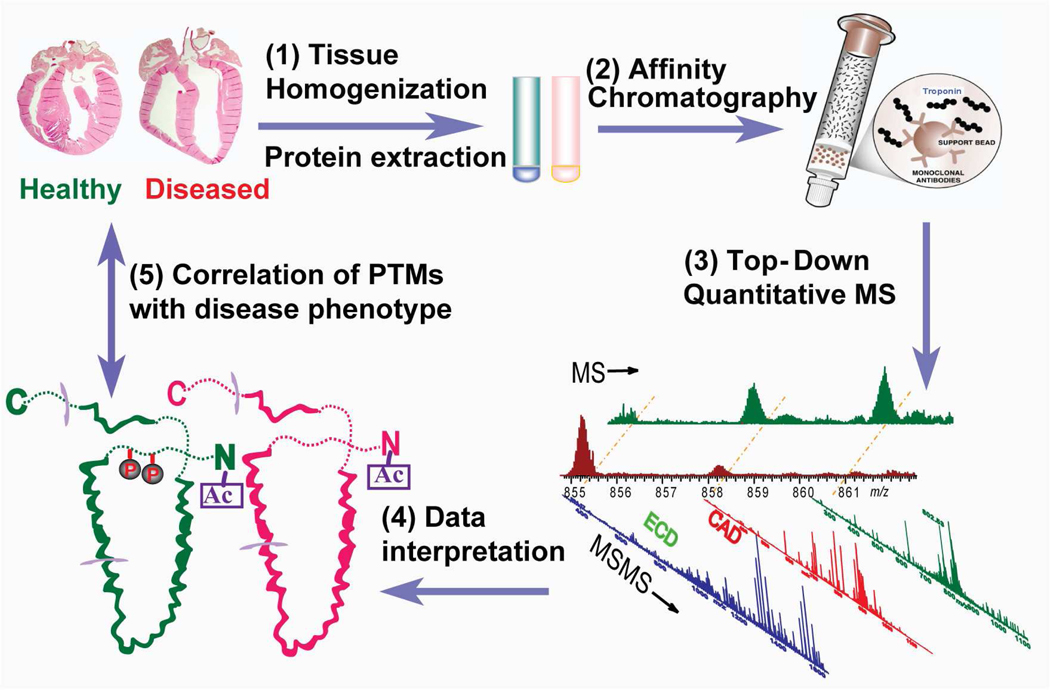
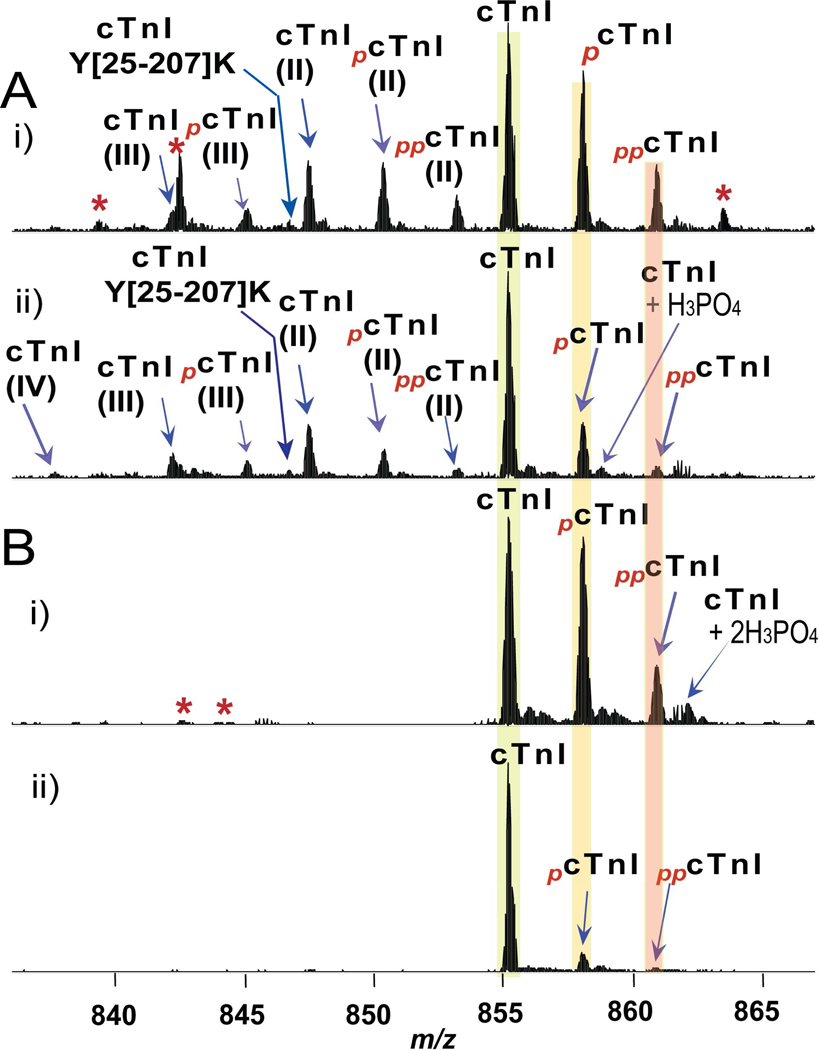
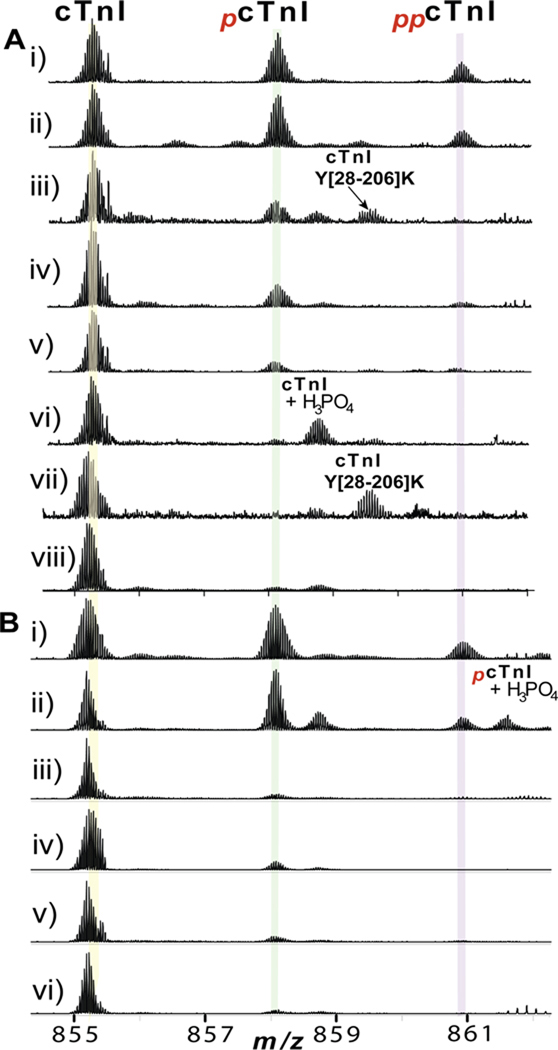
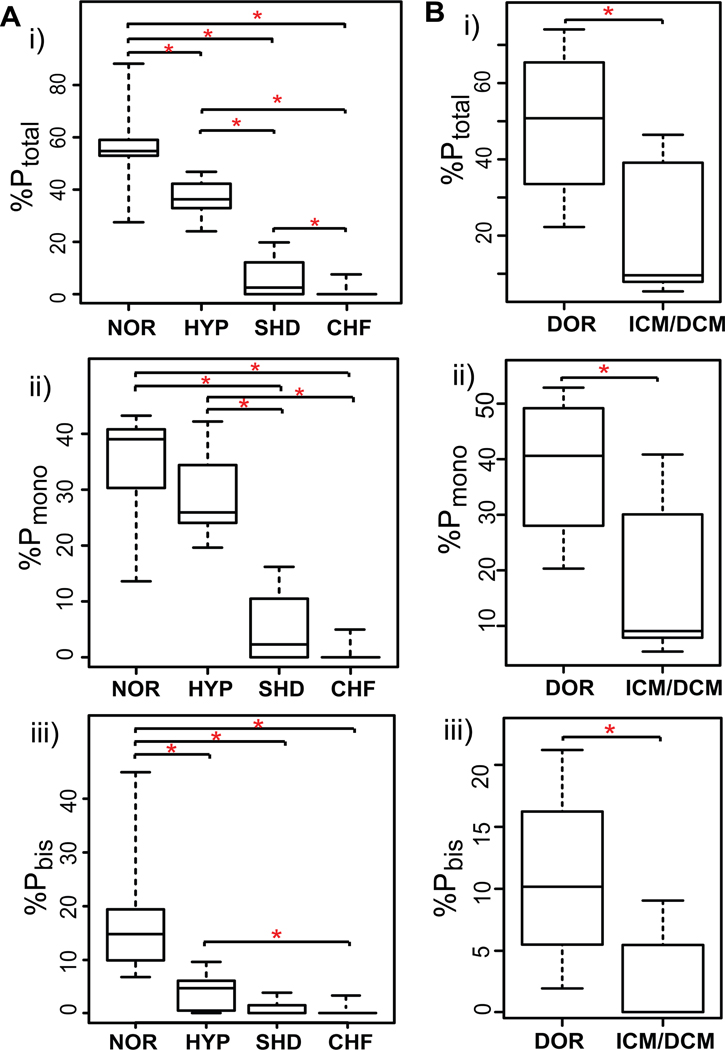
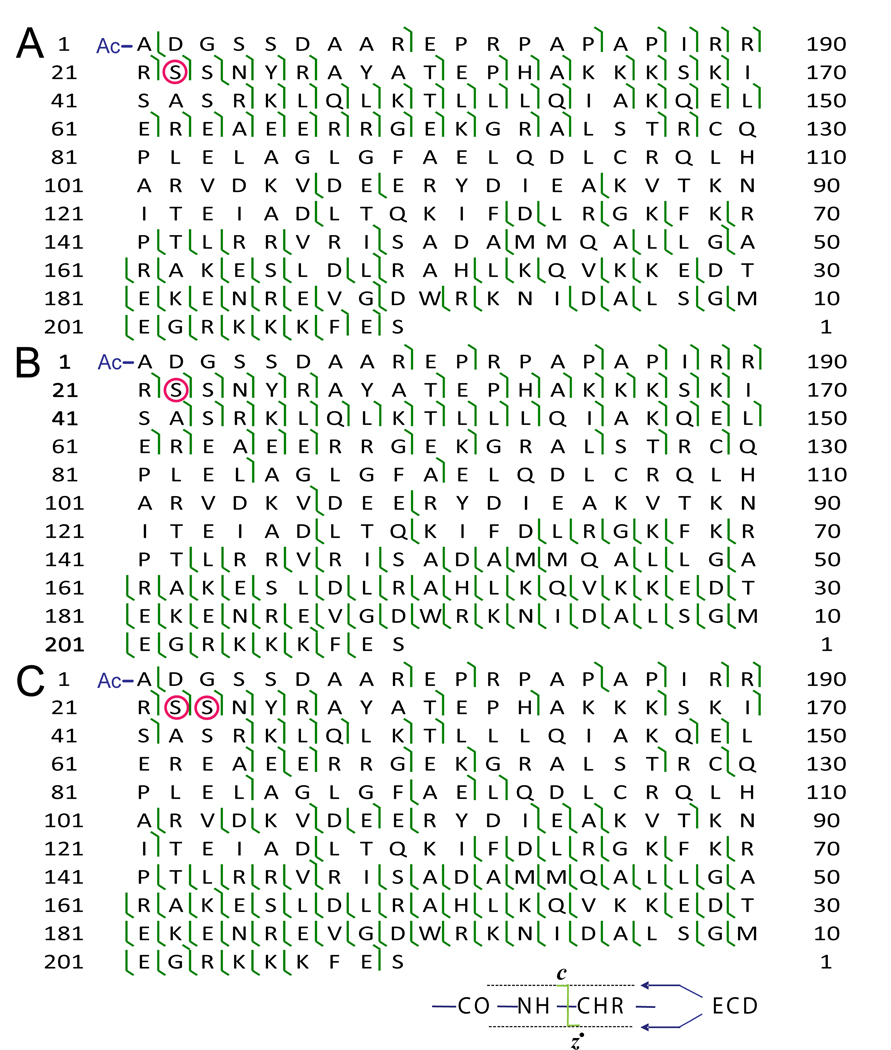
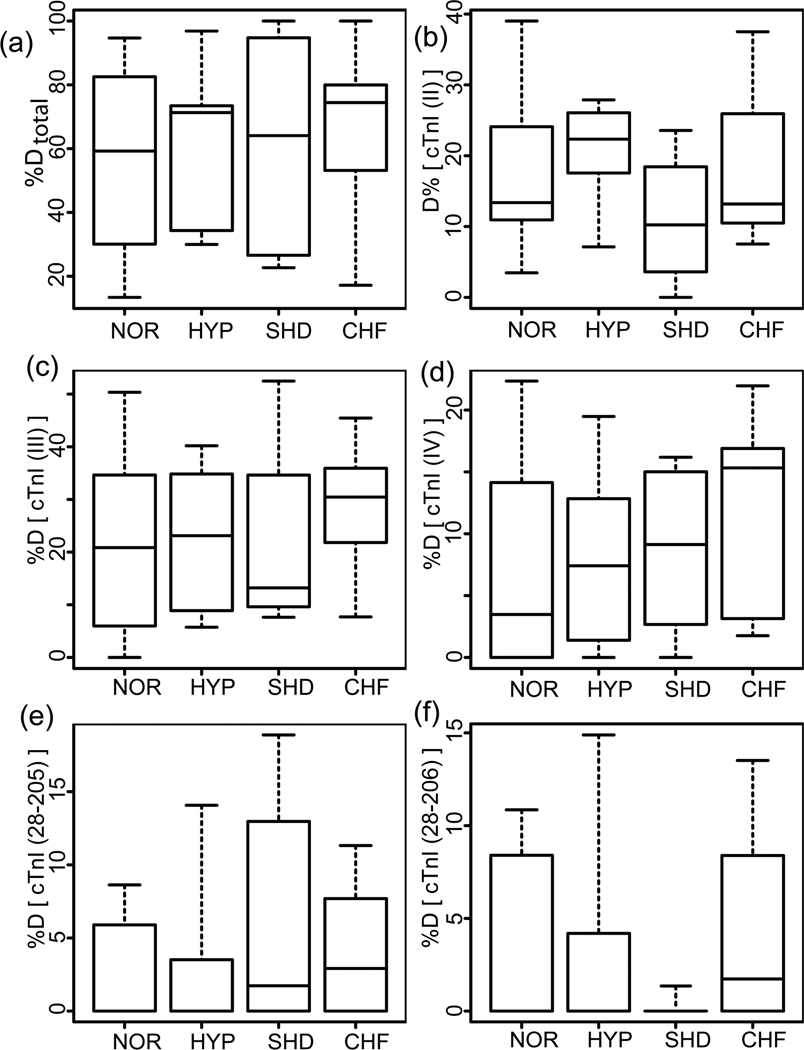
The rapid increase in the prevalence of chronic heart failure (CHF) worldwide underscores an urgent need to identify biomarkers for the early detection of CHF. Post-translational modifications (PTMs) are associated with many critical signaling events during disease progression and thus offer a plethora of candidate biomarkers. We have employed a top-down quantitative proteomics methodology for comprehensive assessment of PTMs in whole proteins extracted from normal and diseased tissues. We systematically analyzed 36 clinical human heart tissue samples and identified phosphorylation of cardiac troponin I (cTnI) as a candidate biomarker for CHF. The relative percentages of the total phosphorylated cTnI forms over the entire cTnI populations (%P(total)) were 56.4 ± 3.5%, 36.9 ± 1.6%, 6.1 ± 2.4%, and 1.0 ± 0.6% for postmortem hearts with normal cardiac function (n = 7), early stage of mild hypertrophy (n = 5), severe hypertrophy/dilation (n = 4), and end-stage CHF (n = 6), respectively. In fresh transplant samples, the %P(total) of cTnI from nonfailing donor (n = 4), and end-stage failing hearts (n = 10) were 49.5 ± 5.9% and 18.8 ± 2.9%, respectively. Top-down MS with electron capture dissociation unequivocally localized the altered phosphorylation sites to Ser22/23 and determined the order of phosphorylation/dephosphorylation. This study represents the first clinical application of top-down MS-based quantitative proteomics for biomarker discovery from tissues, highlighting the potential of PTMs as disease biomarkers.
Figures
Comment in
-
Modified troponin I as a candidate marker for chronic heart failure: a top-down perspective.Circ Cardiovasc Genet. 2011 Oct;4(5):579-80. doi: 10.1161/CIRCGENETICS.111.961573. Circ Cardiovasc Genet. 2011. PMID: 22010167 No abstract available.
References
-
- Mudd JO, Kass DA. Tackling heart failure in the twenty-first century. Nature. 2008;451(7181):919–928. - PubMed
-
- Yach D, Hawkes C, Gould CL, Hofman KJ. The global burden of chronic diseases - Overcoming impediments to prevention and control. J. Am. Med. Assoc. 2004;291(21):2616–2622. - PubMed
-
- de Couto G, Ouzounian M, Liu PP. Early detection of myocardial dysfunction and heart failure. Nat. Rev. Cardiol. 2010;7(6):334–344. - PubMed
-
- Surinova S, Schiess R, Hu¨ttenhain R, Cerciello F, Wollscheid B, Aebersold R. On the Development of Plasma Protein Biomarkers. J. Proteome Res. 2011;10:5–16. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
