

Active albuterol or placebo, sham acupuncture, or no intervention in asthma
- PMID: 21751905
- PMCID: PMC3154208
- DOI: 10.1056/NEJMoa1103319
Active albuterol or placebo, sham acupuncture, or no intervention in asthma
Abstract
Background: In prospective experimental studies in patients with asthma, it is difficult to determine whether responses to placebo differ from the natural course of physiological changes that occur without any intervention. We compared the effects of a bronchodilator, two placebo interventions, and no intervention on outcomes in patients with asthma.
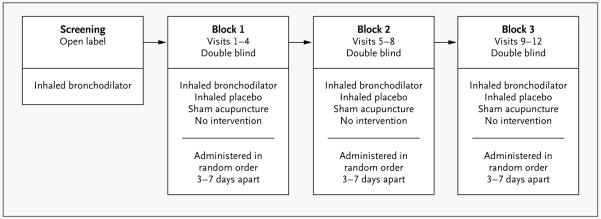
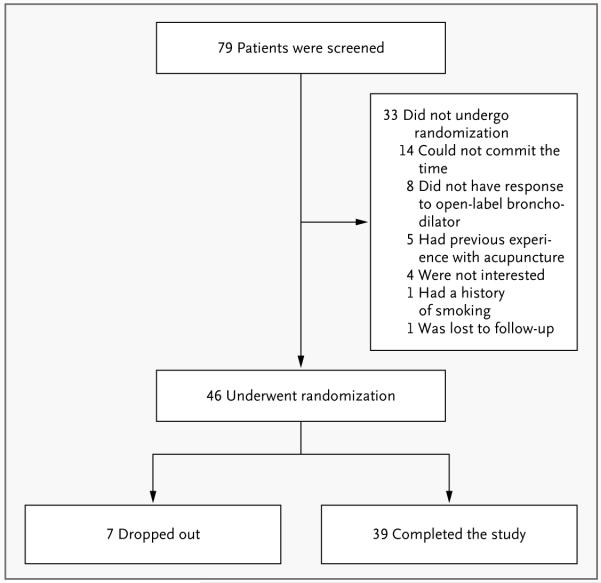
Methods: In a double-blind, crossover pilot study, we randomly assigned 46 patients with asthma to active treatment with an albuterol inhaler, a placebo inhaler, sham acupuncture, or no intervention. Using a block design, we administered one each of these four interventions in random order during four sequential visits (3 to 7 days apart); this procedure was repeated in two more blocks of visits (for a total of 12 visits by each patient). At each visit, spirometry was performed repeatedly over a period of 2 hours. Maximum forced expiratory volume in 1 second (FEV(1)) was measured, and patients' self-reported improvement ratings were recorded.
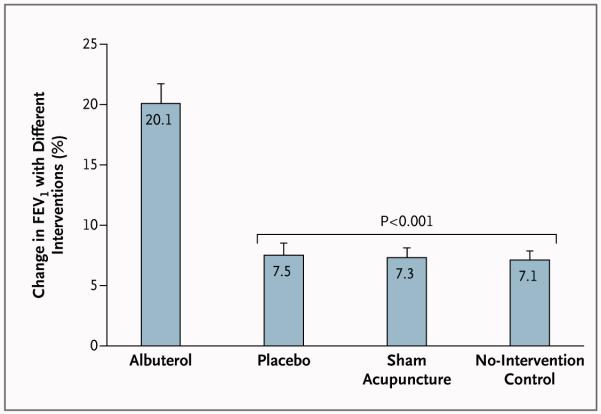
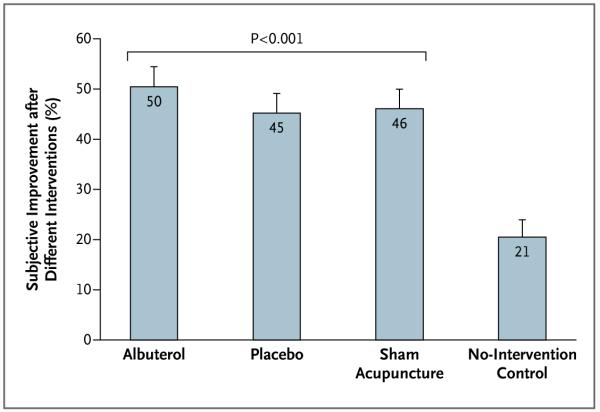
Results: Among the 39 patients who completed the study, albuterol resulted in a 20% increase in FEV(1), as compared with approximately 7% with each of the other three interventions (P<0.001). However, patients' reports of improvement after the intervention did not differ significantly for the albuterol inhaler (50% improvement), placebo inhaler (45%), or sham acupuncture (46%), but the subjective improvement with all three of these interventions was significantly greater than that with the no-intervention control (21%) (P<0.001).
Conclusions: Although albuterol, but not the two placebo interventions, improved FEV(1) in these patients with asthma, albuterol provided no incremental benefit with respect to the self-reported outcomes. Placebo effects can be clinically meaningful and can rival the effects of active medication in patients with asthma. However, from a clinical-management and research-design perspective, patient self-reports can be unreliable. An assessment of untreated responses in asthma may be essential in evaluating patient-reported outcomes. (Funded by the National Center for Complementary and Alternative Medicine.).
Figures
Comment in
-
Meaningful placebos--controlling the uncontrollable.N Engl J Med. 2011 Jul 14;365(2):171-2. doi: 10.1056/NEJMe1104010. N Engl J Med. 2011. PMID: 21751911 No abstract available.
-
Placebo and other interventions in asthma.N Engl J Med. 2011 Oct 13;365(15):1446; author reply 1447. doi: 10.1056/NEJMc1109235. N Engl J Med. 2011. PMID: 21995394 No abstract available.
-
Placebo and other interventions in asthma.N Engl J Med. 2011 Oct 13;365(15):1446; author reply 1447. doi: 10.1056/NEJMc1109235. N Engl J Med. 2011. PMID: 21995395 No abstract available.
References
-
- Temple R, Ellenberg SS. Placebo-controlled trials and active-control trials in the evaluation of new treatments. Part 1: ethical and scientific issues. Ann Intern Med. 2000;133:455–63. - PubMed
-
- Kaptchuk TJ. Powerful placebo: the dark side of the randomised controlled trial. Lancet. 1998;351:1722–5. - PubMed
-
- Hróbjartsson A, Gotzsche PC. Is the placebo powerless? An analysis of clinical trials comparing placebo with no treatment. N Engl J Med. 2001;344:1594–602. - PubMed
-
- Luparello T, Lyons HA, Bleeker ER, McFadden EF., Jr Influence of suggestion on airway reactivity in asthmatic subjects. Psychosom Med. 1968;30:819–25. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical