

Current landscape for T-cell targeting in autoimmunity and transplantation
- PMID: 21751954
- PMCID: PMC3666312
- DOI: 10.2217/imt.11.61
Current landscape for T-cell targeting in autoimmunity and transplantation
Abstract
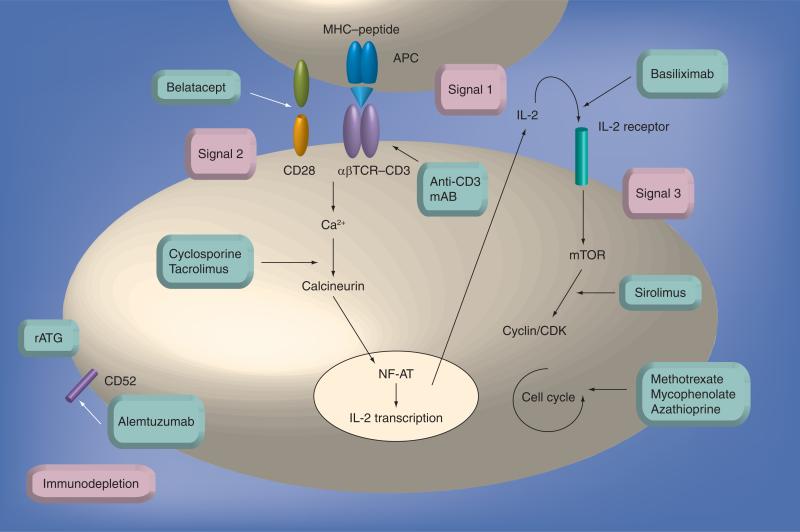
In recent years, substantial advances in T-cell immunosuppressive strategies and their translation to routine clinical practice have revolutionized management and outcomes in autoimmune disease and solid organ transplantation. More than 80 diseases have been considered to have an autoimmune etiology, such that autoimmune-associated morbidity and mortality rank as third highest in developed countries, after cardiovascular diseases and cancer. Solid organ transplantation has become the therapy of choice for many end-stage organ diseases. Short-term outcomes such as patient and allograft survival at 1 year, acute rejection rates, as well as time course of disease progression and symptom control have steadily improved. However, despite the use of newer immunosuppressive drug combinations, improvements in long-term allograft survival and complete resolution of autoimmunity remain elusive. In addition, the chronic use of nonspecifically targeted immunosuppressive drugs is associated with significant adverse effects and increased morbidity and mortality. In this article, we discuss the current clinical tools for immune suppression and attempts to induce long-term T-cell tolerance induction as well as much-needed future approaches to produce more short-acting, antigen-specific agents, which may optimize outcomes in the clinic.
Figures
References
-
- Manilay JO, Waneck GL, Sykes M. Altered expression of Ly-49 receptors on NK cells developing in mixed allogeneic bone marrow chimeras. Int. Immunol. 1998;10(12):1943–1955. - PubMed
-
- Ciancio G, Burke GW, Gaynor JJ, et al. The use of Campath-1H as induction therapy in renal transplantation: preliminary results. Transplantation. 2004;78(3):426–433. - PubMed
-
- Lombardi G, Sidhu S, Batchelor R, Lechler R. Anergic T cells as suppressor cells in vitro. Science. 1994;264(5165):1587–1589. - PubMed
-
- Bishop GA, Sun J, Sheil AG, Mccaughan GW. High-dose/activation-associated tolerance: a mechanism for allograft tolerance. Transplantation. 1997;64(10):1377–1382. - PubMed
-
- Preville X, Flacher M, Lemauff B, et al. Mechanisms involved in antithymocyte globulin immunosuppressive activity in a nonhuman primate model. Transplantation. 2001;71(3):460–468. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical