

Cardiovascular disease by diabetes status in five ethnic minority groups compared to ethnic Norwegians
- PMID: 21752237
- PMCID: PMC3199594
- DOI: 10.1186/1471-2458-11-554
Cardiovascular disease by diabetes status in five ethnic minority groups compared to ethnic Norwegians
Abstract
Background: The population in Norway has become multi-ethnic due to migration from Asia and Africa over the recent decades. The aim of the present study was to explore differences in the self-reported prevalence of cardiovascular disease (CVD) and associated risk factors by diabetes status in five ethnic minority groups compared to ethnic Norwegians.
Methods: Pooled data from three population-based cross-sectional studies conducted in Oslo between 2000 and 2002 was used. Of 54,473 invited individuals 24,749 (45.4%) participated. The participants self-reported health status, underwent a clinical examination and blood samples were drawn. A total of 17,854 individuals aged 30 to 61 years born in Norway, Sri-Lanka, Pakistan, Iran, Vietnam or Turkey were included in the study. Chi-square tests, one-way ANOVAs, ANCOVAs, multiple and logistic regression were used.
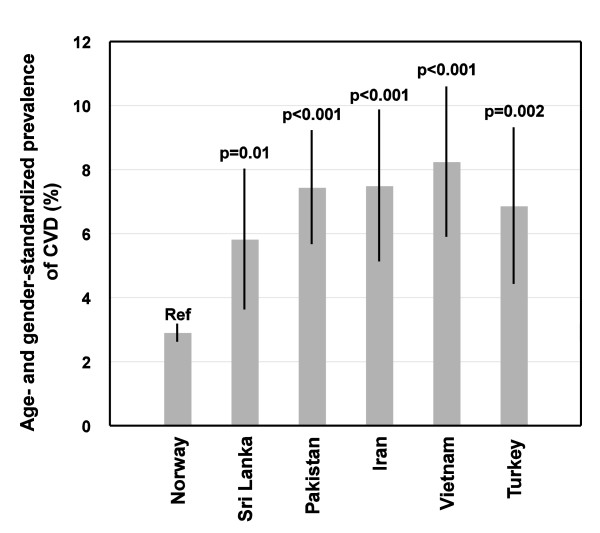
Results: Age- and gender-standardized prevalence of self-reported CVD varied between 5.8% and 8.2% for the ethnic minority groups, compared to 2.9% among ethnic Norwegians (p < 0.001). Prevalence of self-reported diabetes varied from 3.0% to 15.0% for the ethnic minority groups versus 1.8% for ethnic Norwegians (p < 0.001). Among individuals without diabetes, the CVD prevalence was 6.0% versus 2.6% for ethnic minorities and Norwegians, respectively (p < 0.001). Corresponding CVD prevalence rates among individuals with diabetes were 15.3% vs. 12.6% (p = 0.364). For individuals without diabetes, the odds ratio (OR) for CVD in the ethnic minority groups remained significantly higher (range 1.5-2.6) than ethnic Norwegians (p < 0.05), after adjustment for age, gender, education, employment, and body height, except for Turkish individuals. Regardless of diabetes status, obesity and physical inactivity were prevalent in the majority of ethnic minority groups, whereas systolic- and diastolic- blood pressures were higher in Norwegians. In nearly all ethnic groups, individuals with diabetes had higher triglycerides, waist-to-hip ratio (WHR), and body mass index compared to individuals without diabetes. Age, diabetes, hypertension, hypercholesterolemia, and WHR were significant predictors of CVD in both ethnic Norwegians and ethnic minorities, but significant ethnic differences were found for age, diabetes, and hypercholesterolemia.
Conclusions: Ethnic differences in the prevalence of CVD were prominent for individuals without diabetes. Primary CVD prevention including identification of undiagnosed diabetes should be prioritized for ethnic minorities without known diabetes.
Figures

References
-
- Patel JV, Vyas A, Cruickshank JK, Prabhakaran D, Hughes E, Reddy KS, Mackness MI, Bhatnagar D, Durrington PN. Impact of migration on coronary heart disease risk factors: comparison of Gujaratis in Britain and their contemporaries in villages of origin in India. Atherosclerosis. 2006;185:297–306. doi: 10.1016/j.atherosclerosis.2005.06.005. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
