

Qualitative and quantitative skeletal muscle ultrasound in late-onset acid maltase deficiency
- PMID: 21755514
- PMCID: PMC3193541
- DOI: 10.1002/mus.22088
Qualitative and quantitative skeletal muscle ultrasound in late-onset acid maltase deficiency
Abstract
Introduction: Acid maltase deficiency (AMD, or Pompe disease) is an inherited myopathic disorder of glycogen degradation. Diagnosis is often delayed. Muscle ultrasound could improve diagnosis.
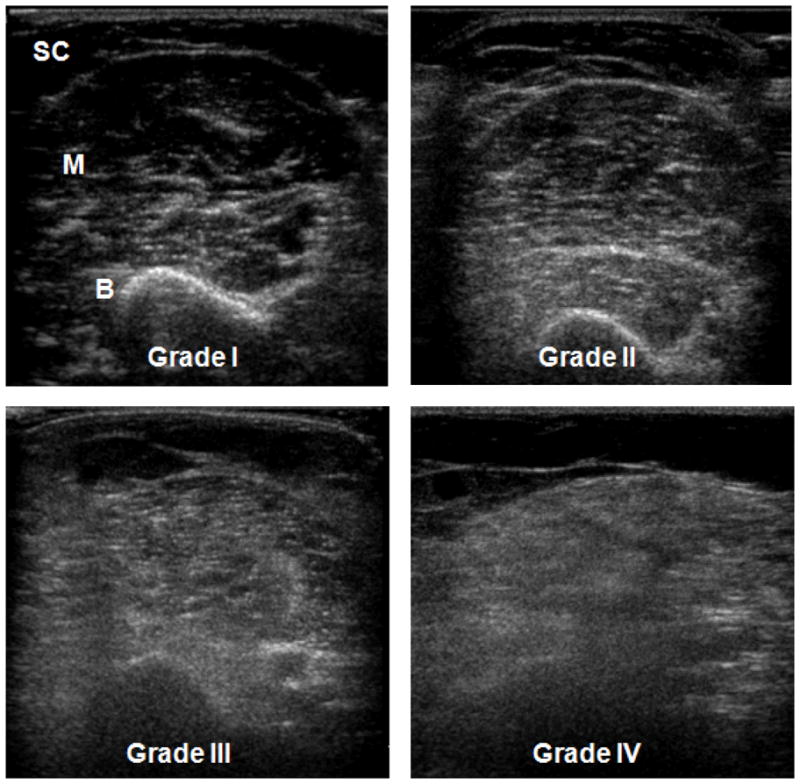
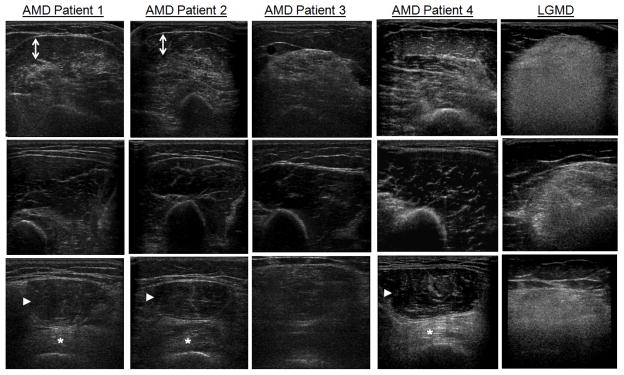
Methods: We compared skeletal muscle ultrasound images from adults with AMD (n = 10) to other myopathies (n = 81) and, in AMD, compared qualitative (Heckmatt) and quantitative (backscatter) ultrasound measurements with strength and function.
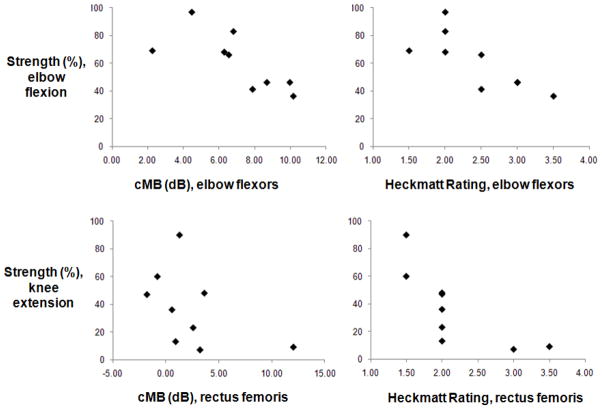
Results: Qualitative ultrasound was abnormal in at least one muscle in all AMD subjects. Ultrasound patterns specific for AMD were: normal triceps brachii despite abnormalities in elbow flexors (89% vs. 17%, P < 0.0001); focal abnormalities affecting deep more than superficial biceps brachii (40% vs. 4%, P = 0.002); and more severe involvement of vastus intermedius than rectus femoris (40 vs. 11%, P = 0.03). In AMD, both qualitative (Heckmatt) and quantitative (backscatter) ultrasound measures increased with decreasing strength and function.
Conclusions: Muscle ultrasound identifies the presence and specific patterns of AMD pathology, measures disease severity, and can help in the diagnosis of AMD.
Copyright © 2011 Wiley Periodicals, Inc.
Figures
References
-
- Martiniuk F, Chen A, Mack A, Arvanitopoulos E, Chen Y, Rom WN, Codd WJ, Hanna B, Alcabes P, Raben N, Plotz P. Carrier frequency for glycogen storage disease type II in New York and estimates of affected individuals born with the disease. Am J Med Genet. 1998;79:69–72. - PubMed
-
- Diagnostic criteria for late-onset (childhood and adult) Pompe disease. Muscle Nerve. 2009;40:149–160. - PubMed
-
- Hagemans ML, Winkel LP, Van Doorn PA, Hop WJ, Loonen MC, Reuser AJ, Van der Ploeg AT. Clinical manifestation and natural course of late-onset Pompe’s disease in 54 Dutch patients. Brain. 2005;128:671–677. - PubMed
-
- Winkel LP, Hagemans ML, van Doorn PA, Loonen MC, Hop WJ, Reuser AJ, van der Ploeg AT. The natural course of non-classic Pompe’s disease; a review of 225 published cases. J Neurol. 2005;252:875–884. - PubMed
-
- van der Ploeg AT, Clemens PR, Corzo D, Escolar DM, Florence J, Groeneveld GJ, Herson S, Kishnani PS, Laforet P, Lake SL, Lange DJ, Leshner RT, Mayhew JE, Morgan C, Nozaki K, Park DJ, Pestronk A, Rosenbloom B, Skrinar A, van Capelle CI, van der Beek NA, Wasserstein M, Zivkovic SA. A randomized study of alglucosidase alfa in late-onset Pompe’s disease. N Engl J Med. 2010;362:1396–1406. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
