

Antiretroviral therapy and the control of HIV-associated tuberculosis. Will ART do it?
- PMID: 21756508
- PMCID: PMC4067901
- DOI: 10.5588/ijtld.10.0483
Antiretroviral therapy and the control of HIV-associated tuberculosis. Will ART do it?
Abstract
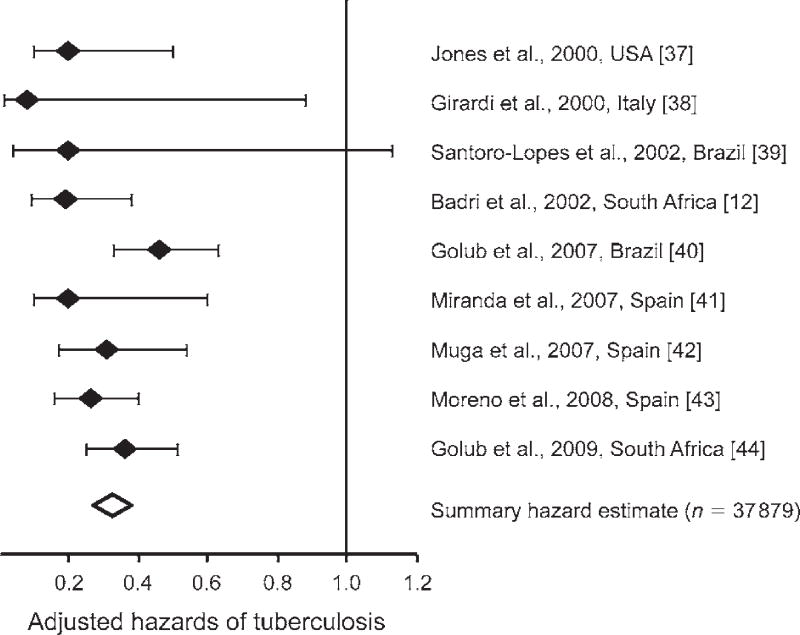
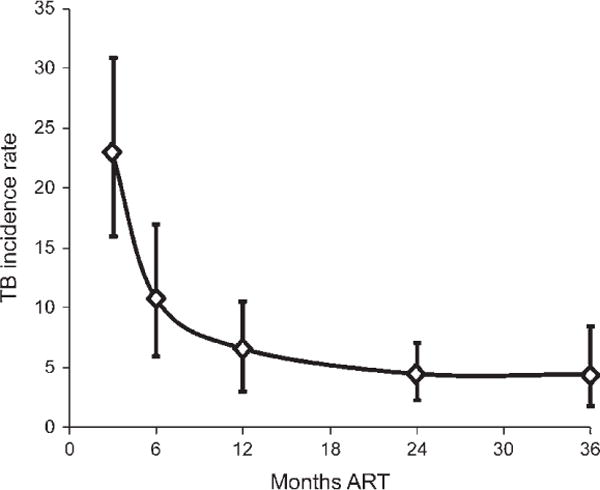
The human immunodeficiency virus (HIV) associated tuberculosis (TB) epidemic remains an enormous challenge to TB control in countries with a high prevalence of HIV. In their 1999 article entitled 'Will DOTS do it?', De Cock and Chaisson questioned whether the World Health Organization's DOTS Strategy could control this epidemic. Data over the past 10 years have clearly shown that DOTS is insufficient as a single TB control intervention in such settings because it does not address the fundamental epidemiological interactions between TB and HIV. Immunodeficiency is a principal driver of this epidemic, and the solution must therefore include immune recovery using antiretroviral therapy (ART). Thus, in the era of global ART scale-up, we now ask the question, 'Will ART do it?' ART reduces the risk of TB by 67% (95%CI 61-73), halves TB recurrence rates, reduces mortality risk by 64-95% in cohorts and prolongs survival in patients with HIV-associated drug-resistant TB. However, the cumulative lifetime risk of TB in HIV-infected individuals is a function of time spent at various CD4-defined levels of risk, both before and during ART. Current initiation of ART at low CD4 cell counts (by which time much HIV-associated TB has already occurred) and low effective coverage greatly undermine the potential impact of ART at a population level. Thus, while ART has proven a critical intervention for case management of HIV-associated TB, much of its preventive potential for TB control is currently being squandered. Much earlier ART initiation with high coverage is required if ART is to substantially influence the incidence of TB.
Figures
References
-
- United Nations. The Millennium Development Goals report 2008. New York, NY, USA: United Nations; 2008. http://www.un.org/millenniumgoals/. Accessed February 2011.
-
- World Health Organization. Global plan to stop TB 2006–2015. Geneva, Switzerland: WHO; Stop TB Partnership. http://www.stoptb.org/global/plan/ Accessed February 2011.
-
- World Health Organization. Epidemiology, strategy, financing. Geneva, Switzerland: WHO; 2009. Global tuberculosis control 2009. (WHO/HTM/TB/2009.411). http://www.who.int/tb/publications/global_report/2009/en/index.html Accessed February 2011.
-
- De Cock KM, Chaisson RE. Will DOTS do it? A reappraisal of tuberculosis control in countries with high rates of HIV infection. Int J Tuberc Lung Dis. 1999;3:457–465. - PubMed
-
- World Health Organization. Report of a joint WHO HIV/AIDS and TB Department meeting, 2008. Geneva, Switzerland: WHO; 2008. WHO Three I’s meeting. http://www.who.int/hiv/pub/meetingreports/WHO_3Is_meeting_report.pdf Accessed February 2011.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
