

Tuberculosis in HIV programmes in lower-income countries: practices and risk factors
- PMID: 21756512
- PMCID: PMC3140103
- DOI: 10.5588/ijtld.10.0249
Tuberculosis in HIV programmes in lower-income countries: practices and risk factors
Abstract
Background: Tuberculosis (TB) is a common diagnosis in human immunodeficiency virus (HIV) infected patients on antiretroviral treatment (ART).
Objective: To describe TB-related practices in ART programmes in lower-income countries and identify risk factors for TB in the first year of ART.
Methods: Programme characteristics were assessed using standardised electronic questionnaire. Patient data from 2003 to 2008 were analysed and incidence rate ratios (IRRs) calculated using Poisson regression models.
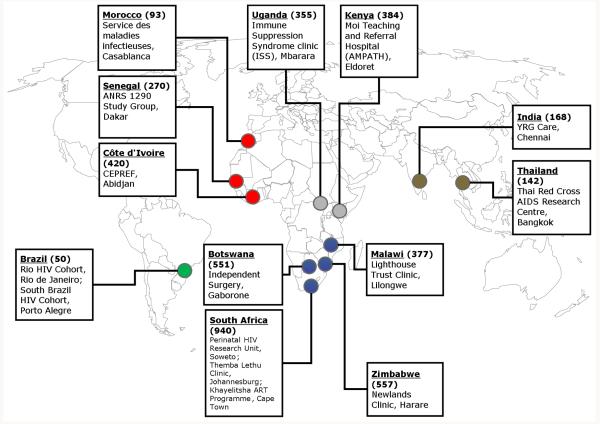
Results: Fifteen ART programmes in 12 countries in Africa, South America and Asia were included. Chest X-ray, sputum microscopy and culture were available free of charge in respectively 13 (86.7%), 14 (93.3%) and eight (53.3%) programmes. Eight sites (53.3%) used directly observed treatment and five (33.3%) routinely administered isoniazid preventive treatment (IPT). A total of 19 413 patients aged ≥ 16 years contributed 13,227 person-years of follow-up; 1081 new TB events were diagnosed. Risk factors included CD4 cell count (>350 cells/μl vs. <25 cells/μl, adjusted IRR 0.46, 95%CI 0.33-0.64, P < 0.0001), sex (women vs. men, adjusted IRR 0.77, 95%CI 0.68-0.88, P = 0.0001) and use of IPT (IRR 0.24, 95%CI 0.19-0.31, P < 0.0001).
Conclusions: Diagnostic capacity and practices vary widely across ART programmes. IPT prevented TB, but was used in few programmes. More efforts are needed to reduce the burden of TB in HIV co-infected patients in lower income countries.
Figures

Comment in
-
Pre-screening with GeneXpert® MTB/RIF may increase use of isoniazid preventive therapy in antiretroviral programmes.Int J Tuberc Lung Dis. 2011 Sep;15(9):1272-3; author reply 1273-4. doi: 10.5588/ijtld.11.0407. Int J Tuberc Lung Dis. 2011. PMID: 21943860 No abstract available.
References
-
- Selwyn PA, Alcabes P, Hartel D, Buono D, Schoenbaum EE, Klein RS, et al. Clinical manifestations and predictors of disease progression in drug users with human immunodeficiency virus infection. N Engl J Med. 1992;327(24):1697–1703. - PubMed
-
- Corbett EL, Watt CJ, Walker N, Maher D, Williams BG, Raviglione MC, et al. The growing burden of tuberculosis: global trends and interactions with the HIV epidemic. Arch Intern Med. 2003;163(9):1009–1021. - PubMed
-
- Dye C. Global epidemiology of tuberculosis. Lancet. 2006;367(9514):938–940. - PubMed
-
- Braitstein P, Brinkhof MW, Dabis F, Schechter M, Boulle A, Miotti P, et al. Mortality of HIV-1-infected patients in the first year of antiretroviral therapy: comparison between low-income and high-income countries. Lancet. 2006;367(9513):817–824. - PubMed
-
- World Health Organization . Scaling up priority HIV/AIDS interventions in the health sector. 2009 Progress Report. World Health Organization; Geneva: [Accessed 23 September 2010]. 2009. Towards universal access. Available from http://www.who.int/hiv/pub/2009progressreport/en/index.html.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
