

Current and future management of bilateral loss of vestibular sensation - an update on the Johns Hopkins Multichannel Vestibular Prosthesis Project
- PMID: 21756683
- PMCID: PMC3270064
- DOI: 10.1179/146701010X12726366068454
Current and future management of bilateral loss of vestibular sensation - an update on the Johns Hopkins Multichannel Vestibular Prosthesis Project
Abstract
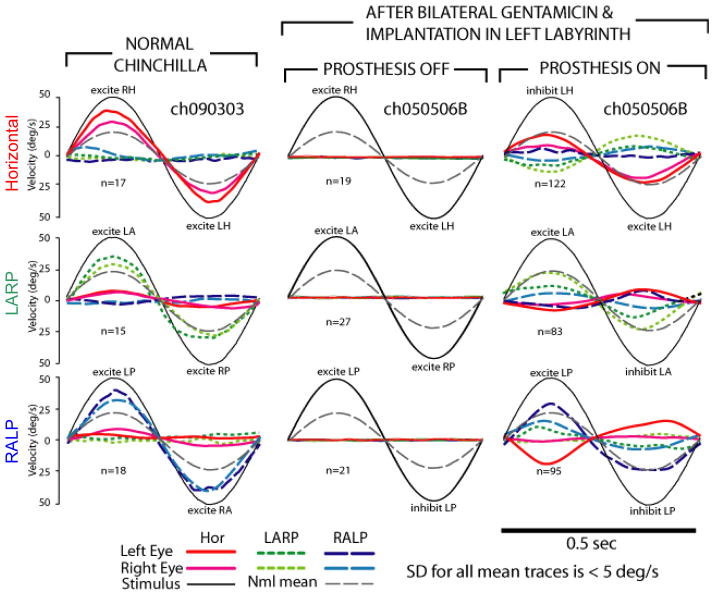
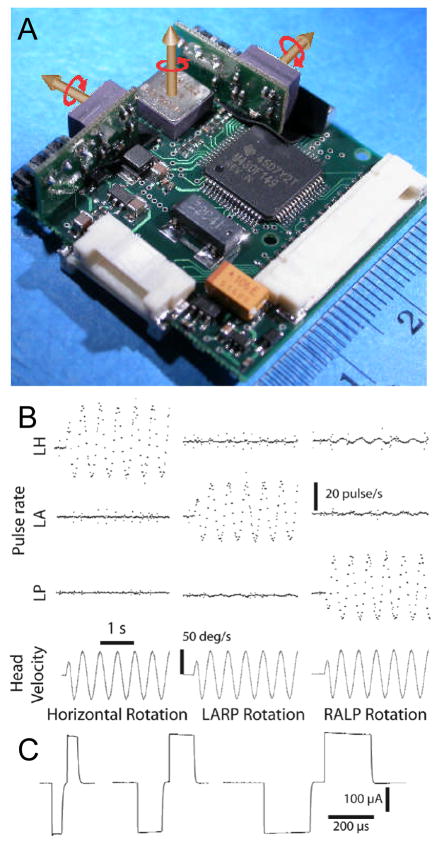
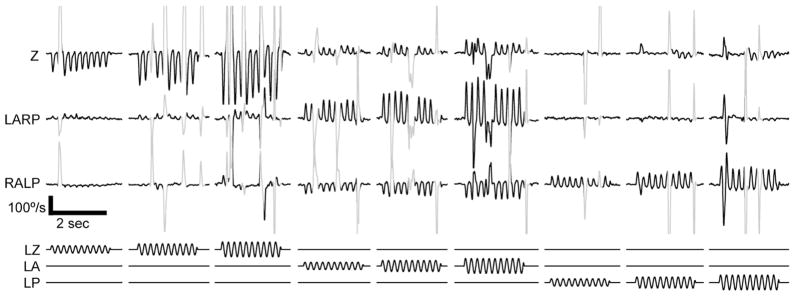
Bilateral loss of vestibular sensation can disable individuals whose vestibular hair cells are injured by ototoxic medications, infection, Ménière's disease or other insults to the labyrinth including surgical trauma during cochlear implantation. Without input to vestibulo-ocular and vestibulo-spinal reflexes that normally stabilize the eyes and body, affected patients suffer blurred vision during head movement, postural instability, and chronic disequilibrium. While individuals with some residual sensation often compensate for their loss through rehabilitation exercises, those who fail to do so are left with no adequate treatment options. An implantable neuroelectronic vestibular prosthesis that emulates the normal labyrinth by sensing head movement and modulating activity on appropriate branches of the vestibular nerve could significantly improve quality of life for these otherwise chronically dizzy patients. This brief review describes the impact and current management of bilateral loss of vestibular sensation, animal studies supporting the feasibility of prosthetic vestibular stimulation, and a vestibular prosthesis designed to restore sensation of head rotation in all directions. Similar to a cochlear implant in concept and size, the Johns Hopkins Multichannel Vestibular Prosthesis (MVP) includes miniature gyroscopes to sense head rotation, a microcontroller to process inputs and control stimulus timing, and current sources switched between pairs of electrodes implanted within the vestibular labyrinth. In rodents and rhesus monkeys rendered bilaterally vestibulardeficient via treatment with gentamicin and/or plugging of semicircular canals, the MVP partially restores the vestibulo-ocular reflex for head rotations about any axis of rotation in 3-dimensional space. Our efforts now focus on addressing issues prerequisite to human implantation, including refinement of electrode designs and surgical technique to enhance stimulus selectivity and preserve cochlear function, optimization of stimulus protocols, and reduction of device size and power consumption.
Figures
References
-
- Abadie V, Wiener-Vacher S, Morisseau-Durand MP, Poree C, Amiel J, Amanou L, Peigne C, Lyonnet S, Manac’h Y. Vestibular anomalies in CHARGE syndrome: investigations on and consequences for postural development. Eur J Pediatr. 2000;159:569–574. - PubMed
-
- Brown KE, Whitney SL, Wrisley DM, Furman JM. Physical therapy outcomes for persons with bilateral vestibular loss. Laryngoscope. 2001;111:1812–1817. - PubMed
-
- Chiang B, Fridman GY, Della Santina CC. Enhancements to the Johns Hopkins Multi-Channel Vestibular Prosthesis yield reduced size, extended battery life, current steering and wireless control. Abst #213, Assoc for Research in Otolaryngology Ann Mtg (ARO); 2009.2009.
-
- Davidovics NS, Fridman GY, Della Santina CC. Effects of Stimulus Pulse Parameters on Eye Movement Responses to Stimulation Delivered by a Vestibular Prosthesis. ARO; 2010.2010.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous