

LV thrombus detection by routine echocardiography: insights into performance characteristics using delayed enhancement CMR
- PMID: 21757159
- PMCID: PMC3724234
- DOI: 10.1016/j.jcmg.2011.03.017
LV thrombus detection by routine echocardiography: insights into performance characteristics using delayed enhancement CMR
Abstract
Objectives: This study sought to evaluate performance characteristics of routine echo for left ventricular thrombus (LVT).
Background: Although the utility of dedicated echocardiography (echo) for LVT is established, echo is widely used as a general test for which LVT is rarely the primary indication. We used delayed-enhancement cardiac magnetic resonance (DE-CMR) as a reference to evaluate LVT detection by routine echo.
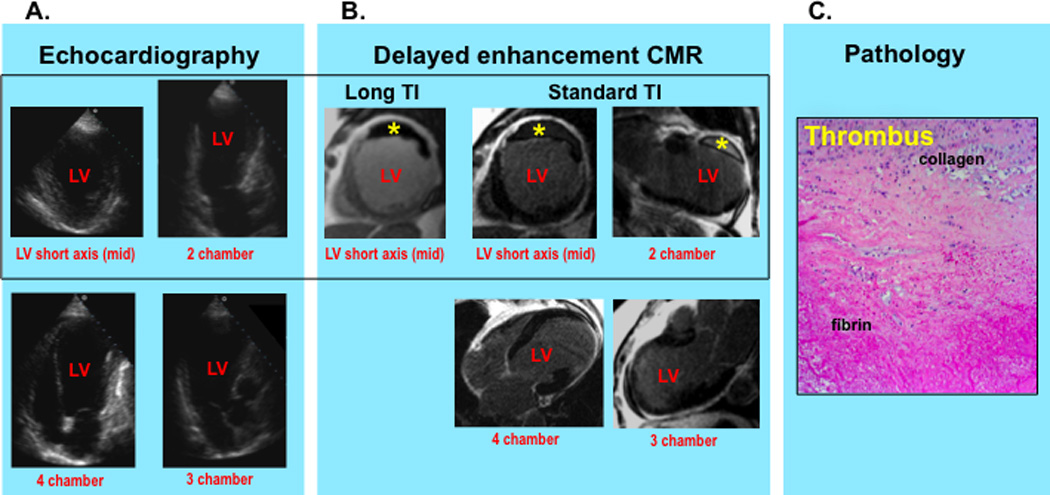
Methods: Dedicated LVT assessment using DE-CMR was prospectively performed in patients with left ventricular systolic dysfunction. Echoes were done as part of routine clinical care. Echo and CMR were independently read for LVT and related indexes of LVT size, shape, and image quality/diagnostic confidence. Follow-up was done for embolic events and pathology validation of LVT.
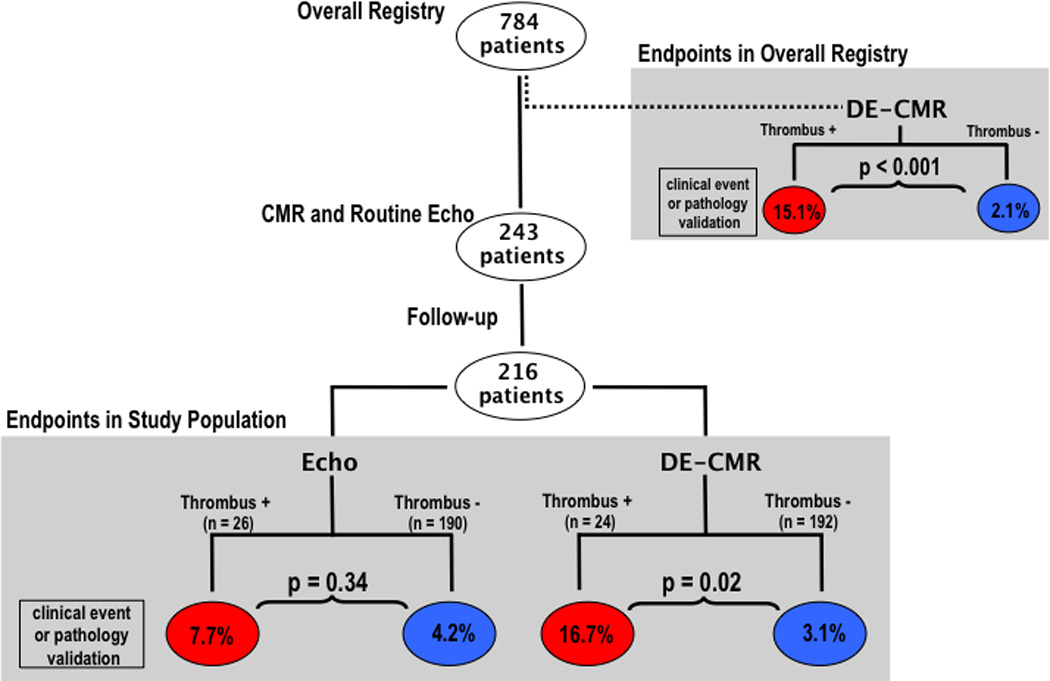
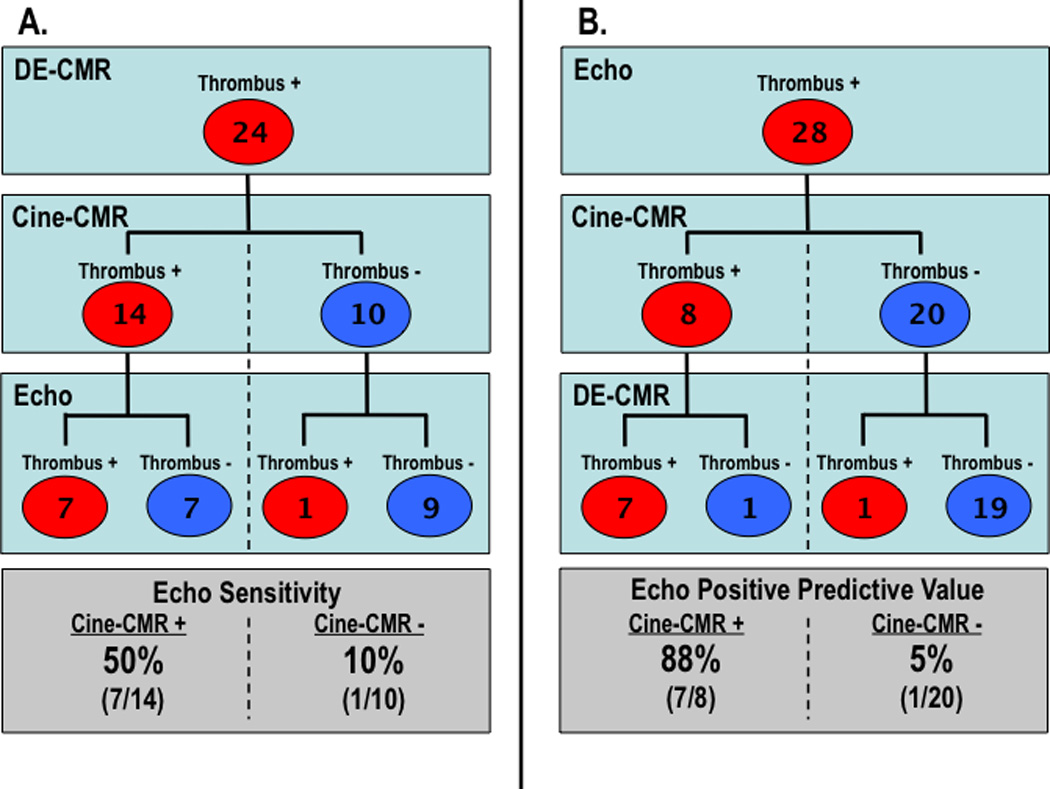
Results: In this study, 243 patients had routine clinical echo and dedicated CMR within 1 week without intervening events. Follow-up supported DE-CMR as a reference standard, with >5-fold difference in endpoints between patients with versus without LVT by DE-CMR (p = 0.02). LVT prevalence was 10% by DE-CMR. Echo contrast was used in 4% of patients. Echo sensitivity and specificity were 33% and 91%, with positive and negative predictive values of 29% and 93%. Among patients with possible LVT as the clinical indication for echo, sensitivity and positive predictive value were markedly higher (60%, 75%). Regarding sensitivity, echo performance related to LVT morphology and mirrored cine-CMR, with protuberant thrombus typically missed when small (p ≤ 0.02). There was also a strong trend to miss mural thrombus irrespective of size (p = 0.06). Concerning positive predictive value, echo performance related to image quality, with lower diagnostic confidence scores for echoes read positive for LVT in discordance with DE-CMR compared with echoes concordant with DE-CMR (p < 0.02).
Conclusions: Routine echo with rare contrast use can yield misleading results concerning LVT. Echo performance is improved when large protuberant thrombus is present and when the clinical indication is specifically for LVT assessment.
Copyright © 2011 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Drs Kim and Judd are inventors of a US patent on Delayed Enhancement MRI, which is owned by Northwestern University. Dr Weinsaft is a recipient of a research grant from Lantheus Medical Imaging on LV thrombus (echo contrast manufacturer).
Figures
Comment in
-
Detecting LV thrombi: "T'ain't what you do (it's the way that you do it)".JACC Cardiovasc Imaging. 2011 Jul;4(7):713-5. doi: 10.1016/j.jcmg.2011.05.002. JACC Cardiovasc Imaging. 2011. PMID: 21757160 No abstract available.
References
-
- Cheitlin MD, Armstrong WF, Aurigemma GP, Beller GA, Bierman FZ, Davis JL, Douglas PS, Faxon DP, Gilliam LD, Kimball TR, Kussmaul WG, Pearlman AS, Philbrick JT, Rakowski H, Thys DM. ACC/AHA/ASE 2003 guideline update for the clinical application of echocardiography: a report of the Amrican College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/ASE Committee to Update the 1997 Guidelines for the Clinical Application of Echocardiography) Circulation. 2003;108:1146–1162. - PubMed
-
- Cheitlin MD, Alpert JS, Armstrong WF, Aurigemma GP, Beller GA, Bierman FZ, Davidson TW, Davis JL, Douglas PS, Gillam LD. ACC/AHA Guidelines for the Clinical Application of Echocardiography. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Clinical Application of Echocardiography). Developed in collaboration with the American Society of Echocardiography. Circulation. 1997;95(6):1686–1744. - PubMed
-
- Visser CA, Kan G, David GK, Lie KI, Durrer D. Two dimensional echocardiography in the diagnosis of left ventricular thrombus. A prospective study of 67 patients with anatomic validation. Chest. 1983;83(2):228–232. - PubMed
-
- Ezekowitz MD, Wilson DA, Smith EO, Burow RD, Harrison LH, Jr, Parker DE, Elkins RC, Peyton M, Taylor FB. Comparison of Indium-111 platelet scintigraphy and two-dimensional echocardiography in the diagnosis of left ventricular thrombi. N Engl J Med. 1982;306(25):1509–1513. - PubMed
-
- Stratton JR, Lighty GW, Jr, Pearlman AS, Ritchie JL. Detection of left ventricular thrombus by two-dimensional echocardiography: sensitivity, specificity, and causes of uncertainty. Circulation. 1982;66(1):156–166. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
