

Urinary biomarkers and renal recovery in critically ill patients with renal support
- PMID: 21757640
- PMCID: PMC3156420
- DOI: 10.2215/CJN.11261210
Urinary biomarkers and renal recovery in critically ill patients with renal support
Abstract
Background and objectives: Despite significant advances in the epidemiology of acute kidney injury (AKI), prognostication remains a major clinical challenge. Unfortunately, no reliable method to predict renal recovery exists. The discovery of biomarkers to aid in clinical risk prediction for recovery after AKI would represent a significant advance over current practice.
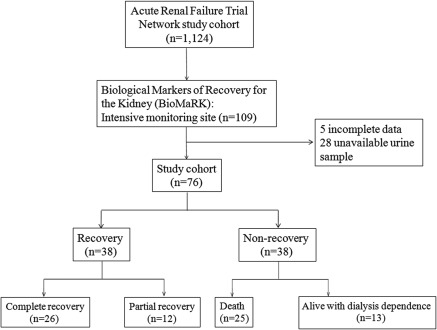
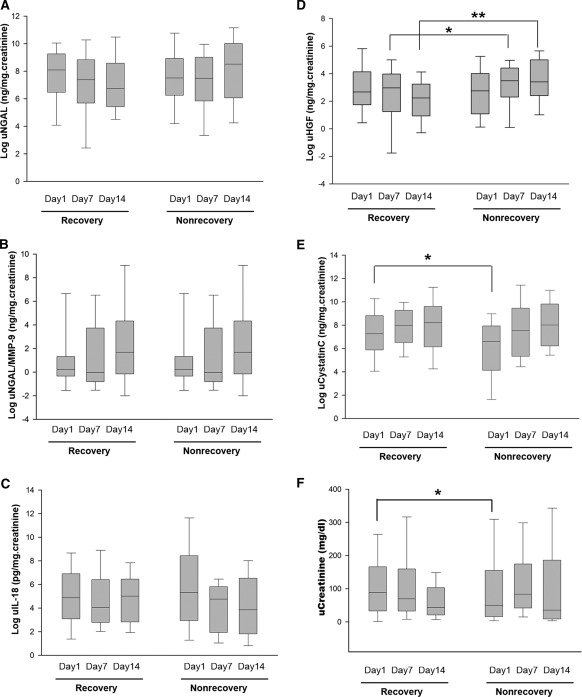
Design, setting, participants, & measurements: We conducted the Biological Markers of Recovery for the Kidney study as an ancillary to the Acute Renal Failure Trial Network study. Urine samples were collected on days 1, 7, and 14 from 76 patients who developed AKI and received renal replacement therapy (RRT) in the intensive care unit. We explored whether levels of urinary neutrophil gelatinase-associated lipocalin (uNGAL), urinary hepatocyte growth factor (uHGF), urinary cystatin C (uCystatin C), IL-18, neutrophil gelatinase-associated lipocalin/matrix metalloproteinase-9, and urine creatinine could predict subsequent renal recovery.
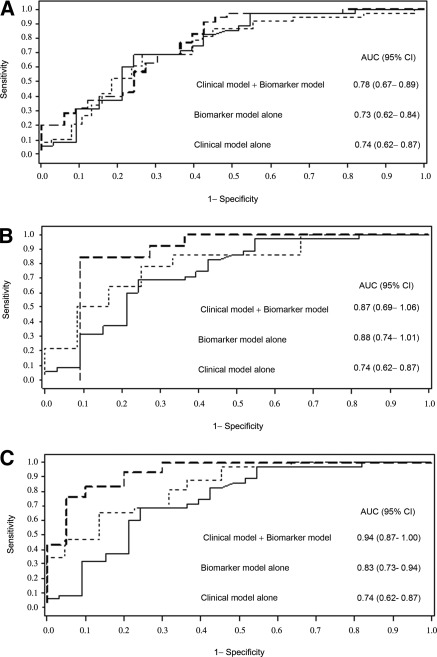
Results: We defined renal recovery as alive and free of dialysis at 60 days from the start of RRT. Patients who recovered had higher uCystatin C on day 1 (7.27 versus 6.60 ng/mg·creatinine) and lower uHGF on days 7 and 14 (2.97 versus 3.48 ng/mg·creatinine; 2.24 versus 3.40 ng/mg·creatinine). For predicting recovery, decreasing uNGAL and uHGF in the first 14 days was associated with greater odds of renal recovery. The most predictive model combined relative changes in biomarkers with clinical variables and resulted in an area under the receiver-operator characteristic curve of 0.94.
Conclusions: We showed that a panel of urine biomarkers can augment clinical risk prediction for recovery after AKI.
Figures
References
-
- Palevsky PM, Zhang JH, O'Connor TZ, Chertow GM, Crowley ST, Choudhury D, Finkel K, Kellum JA, Paganini E, Schein RM, Smith MW, Swanson KM, Thompson BT, Vijayan A, Watnick S, Star RA, Peduzzi P: Intensity of renal support in critically ill patients with acute kidney injury. N Engl J Med 359: 7–20, 2008 - PMC - PubMed
-
- Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, Morgera S, Schetz M, Tan I, Bouman C, Macedo E, Gibney N, Tolwani A, Ronco C: Acute renal failure in critically ill patients: A multinational, multicenter study. JAMA 294: 813–818, 2005 - PubMed
-
- Manns B, Doig CJ, Lee H, Dean S, Tonelli M, Johnson D, Donaldson C: Cost of acute renal failure requiring dialysis in the intensive care unit: Clinical and resource implications of renal recovery. Crit Care Med 31: 449–455, 2003 - PubMed
-
- Supavekin S, Zhang W, Kucherlapati R, Kaskel FJ, Moore LC, Devarajan P: Differential gene expression following early renal ischemia/reperfusion. Kidney Int 63: 1714–1724, 2003 - PubMed
-
- Mishra J, Ma Q, Kelly C, Mitsnefes M, Mori K, Barasch J, Devarajan P: Kidney NGAL is a novel early marker of acute injury following transplantation. Pediatr Nephrol 21: 856–863, 2006 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
