

Relationship between treatment preference and weight loss in the context of a randomized controlled trial
- PMID: 21760633
- PMCID: PMC3819599
- DOI: 10.1038/oby.2011.216
Relationship between treatment preference and weight loss in the context of a randomized controlled trial
Abstract
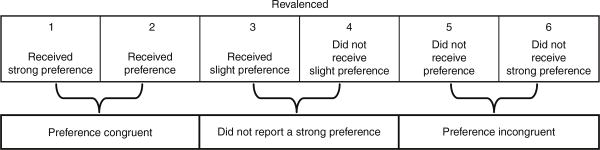
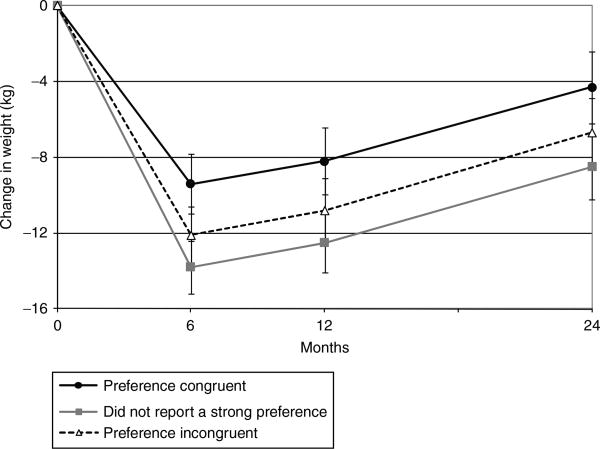
Randomized controlled trials (RCTs) are considered the gold standard used to assess the efficacy of treatment. While a well implemented RCT can produce an unbiased estimate of the relative difference between treatment groups, the generalizability of these findings may be limited. Specific threats to the external validity include treatment preference. The purposes of this study were to: (i) assess whether receiving one's treatment preference was associated with weight loss and retention and (ii) whether receiving one's treatment preference modified the relationship between the treatments and weight loss. Treatment preference was assessed in 250 subjects prior to but independent of randomization into either low-carbohydrate or low-fat diets. Treatment preference was a predictor of weight loss (P = 0.002) but not retention (P = 0.90). Participants who received their preference lost less weight (-7.7 kg, 95% confidence interval (CI): -9.3 to -6.1) than participants who did not receive their preference (-9.7 kg, 95% CI: -11.4 to -8.1) and participants who did not report a strong preference at baseline (-11.2 kg, 95% CI: -12.6 to -9.7) (P = 0.04 and P = 0.0004, respectively). Treatment preference did not modify the effect of the treatment on weight loss. Contrary to conceptual predictions, this study failed to identify an interaction between treatment preference and weight loss in the setting of a randomized trial. Until treatment preference effects are definitively ruled out in this domain, future studies might consider stratifying their randomization procedure by treatment preference rather than excluding participants with strong treatment preferences.
Trial registration: ClinicalTrials.gov NCT00143936.
Figures
References
-
- Rothwell PM. External validity of randomised controlled trials: “to whom do the results of this trial apply?”. Lancet. 2005;365:82–93. - PubMed
-
- Epstein LH. Role of behavior theory in behavioral medicine. J Consult Clin Psychol. 1992;60:493–498. - PubMed
-
- Halpern SD. Evaluating preference effects in partially unblinded, randomized clinical trials. J Clin Epidemiol. 2003;56:109–115. - PubMed
-
- Murray DC. Preferred versus nonpreferred treatment and self-control training versus determination raising as treatments of obesity: a pilot study. Psychol Rep. 1976;38:191–198. - PubMed
-
- Renjilian DA, Perri MG, Nezu AM, et al. Individual versus group therapy for obesity: effects of matching participants to their treatment preferences. J Consult Clin Psychol. 2001;69:717–721. - PubMed
