

Right bundle branch block on alternate beats during acute pulmonary embolism
- PMID: 21762261
- PMCID: PMC6932183
- DOI: 10.1111/j.1542-474X.2011.00434.x
Right bundle branch block on alternate beats during acute pulmonary embolism
Abstract
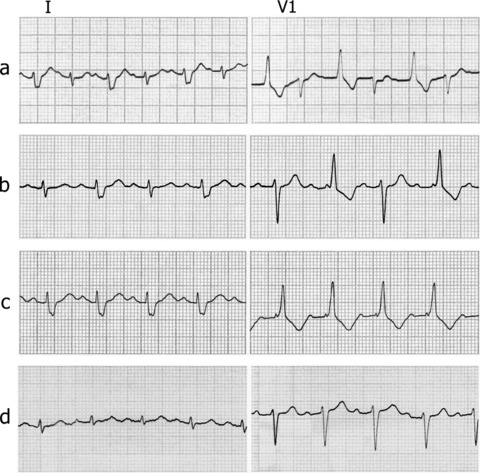
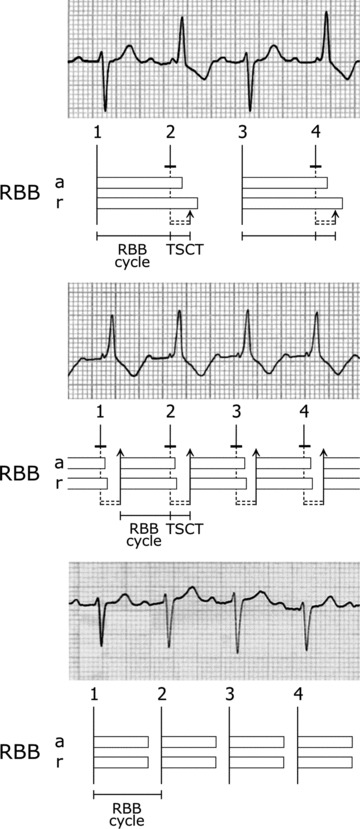
The electrocardiogram of a patient with acute pulmonary embolism showed right bundle branch block (RBBB) on alternate beats; following thrombolysis, the pattern evolved to persistent RBBB and eventually to normal conduction. Analysis of serial tracings suggested that the mechanism of RBBB alternans was tachycardia-dependent bidirectional bundle branch block, caused by prolongation of both anterograde and retrograde refractory periods (RPs) of the right bundle branch (RBB). The sinus impulse found the RBB refractory, and was conducted over the left bundle branch only, depolarizing the left ventricle and then attempting to penetrate retrogradely the RBB; at that time, however, the RBB was still refractory. When a QRS complex had a RBBB configuration, therefore, the RBB was not depolarized; the ensuing sinus impulse found the RBB fully responsive as a consequence of the long period intervening between two successive depolarizations, and resulted in normal intraventricular conduction. With right ventricular afterload decrease, the recovery of RBB anterograde and retrograde excitability was asynchronous, since the retrograde RP became normal earlier than the anterograde one. In accordance with the relatively short retrograde RP, the RBB was retrogradely invaded by the transseptal impulse coming from the left ventricle; this "shifted to the right" the anterograde RP of the RBB. The RBB, thus, was still refractory to the next sinus impulse, and RBBB again occurred; the RBB, thus, was once more depolarized retrogradely, and this led to perpetuation of RBBB. Finally, intraventricular conduction became normal owing to full normalization of RBB anterograde and retrograde refractoriness.
©2011, Wiley Periodicals, Inc.
Figures
References
-
- Cohen HC, D’Cruz I, Arbel ER, et al Tachycardia and bradycardia‐dependent bundle branch block alternans. Clinical observations. Circulation 1977;55:242–246. - PubMed
-
- Cohen HC, D’Cruz IA, Pick A. Effects of stable and changing rates and premature ventricular beats on transient tachycardia‐, pseudobradycardia‐, and bradycardia‐dependent bundle branch block alternans. J Electrocardiol 1979;12:151–156. - PubMed
-
- Carbone V, Tedesco MA. Bundle branch block on alternate beats: By what mechanism? J Electrocardiol 2002;35:147–152. - PubMed
-
- Carbone V, Carerj S, Calabrò MP. Bundle branch block on alternate beats during atrial fibrillation. J Electrocardiol 2004;37:67–72. - PubMed
-
- Nau GJ, Elizari MV, Rosenbaum MB. The different varieties of 2:1 bundle branch block In Rosenbaum MB, Elizari MV. (eds.): Frontiers in Cardiac Electrophysiology. The Hague, Martinus Nijhoff Publishers, 1983, pp. 488–500.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
