

Dynamics of cell-mediated immune responses to cytomegalovirus in pediatric transplantation recipients
- PMID: 21762326
- PMCID: PMC3214231
- DOI: 10.1111/j.1399-3046.2011.01531.x
Dynamics of cell-mediated immune responses to cytomegalovirus in pediatric transplantation recipients
Abstract
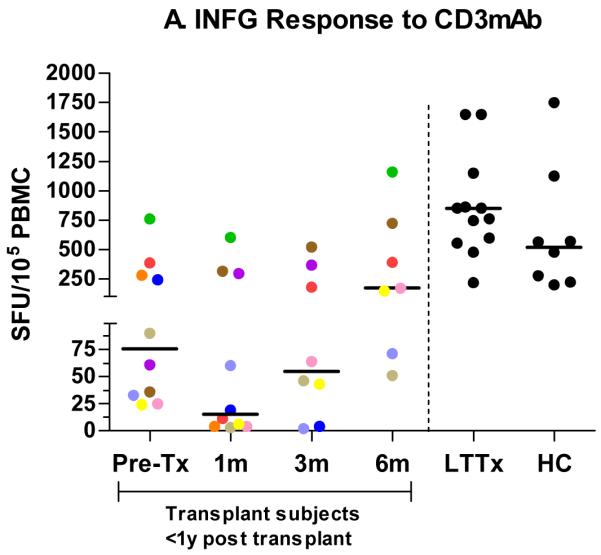
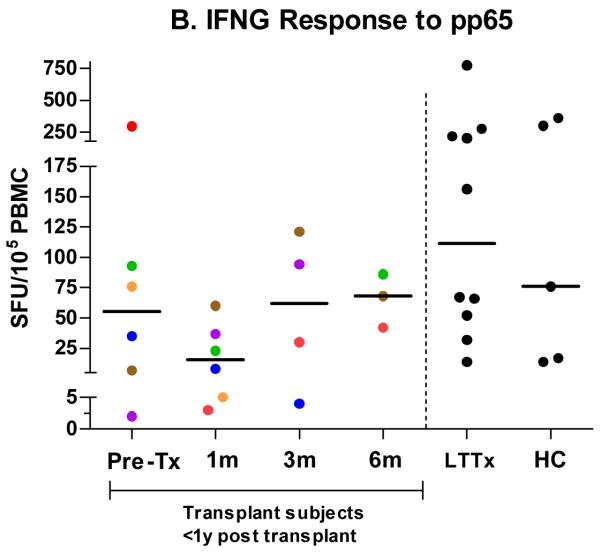
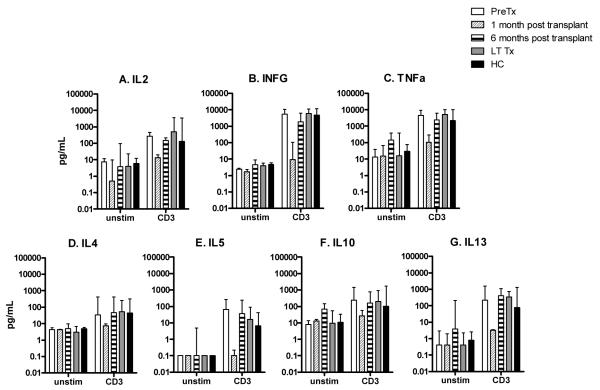
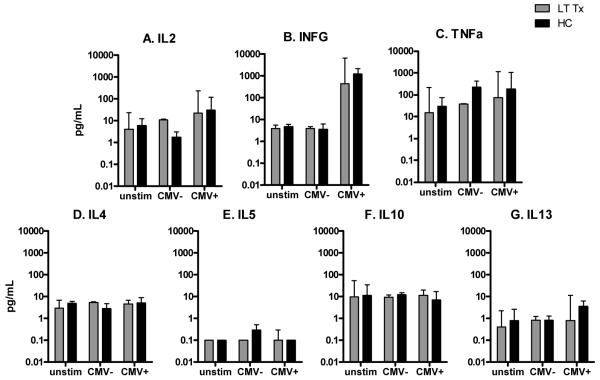
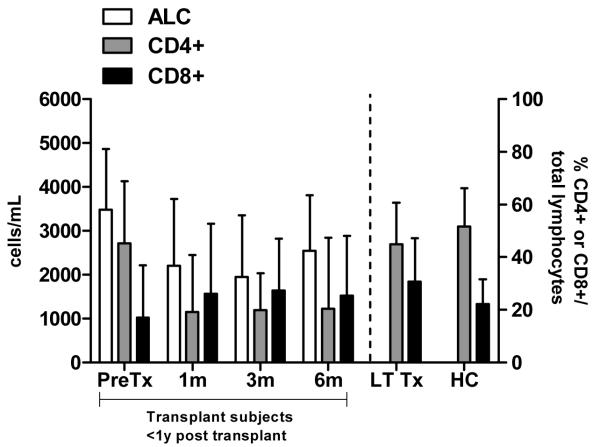
CMI responses, combined with quantification of CMV DNA (DNAemia), may identify transplantation recipients at risk for invasive disease. PBMC were collected in pediatric transplantation candidates at one, three, and six months post-transplant in 10 subjects (six renal, three cardiac, one stem cell) and at single time points in eight HC and 14 children greater than one yr post-transplant (LTTx). Cells were stimulated with anti-CD3mAb or CMV pp65 peptide pools and responses assessed by IFNG enzyme-linked immunosorbent spot assay and cytokine secretion. IFNG responses to anti-CD3mAb were significantly lower pretransplant relative to HC and were further decreased at one and three months post-transplant, but recovered to levels comparable to HC by six months. Responses to pp65 among CMV-seropositive recipients followed a similar pattern but recovered by three months. CMV-seropositive LTTx and HC showed a Th1 cytokine response to pp65 stimulation. Three LTTx subjects developed CMV DNAemia; two demonstrated decreased responses to anti-CD3mAB (and pp65 in the CMV seropositive subject) at the onset of DNAemia, which recovered as DNAemia resolved. Monitoring CMI in children is feasible and may provide an adjunct biomarker to predict CMV progression and recovery.
© 2011 John Wiley & Sons A/S.
Figures
Comment in
-
Cellular immunity to CMV: advancing to the next level.Pediatr Transplant. 2012 Sep;16(6):539-41. doi: 10.1111/j.1399-3046.2011.01637.x. Epub 2012 Jan 19. Pediatr Transplant. 2012. PMID: 22257157 No abstract available.
References
-
- Falagas ME, Paya C, Ruthazer R, et al. Significance of cytomegalovirus for long-term survival after orthotopic liver transplantation: A prospective derivation and validation cohort analysis. Transplantation. 1998;66:1020–1028. - PubMed
-
- Hartmann A, Sagedal S, Hjelmesaeth J. The natural course of cytomegalovirus infection and disease in renal transplant recipients. Transplantation. 2006;82:S15–S17. - PubMed
-
- Von Muller L, Schliep C, Storck M, et al. Severe graft rejection, increased immunosuppression, and active CMV infection in renal transplantation. J Med Virol. 2006;78:394–399. - PubMed
-
- Arend SM, Westendorp RG, Kroon FP, et al. Rejection treatment and cytomegalovirus infection as risk factors for Pneumocystis carinii pneumonia in renal transplant recipients. Clin Infect Dis. 1996;22:920–925. - PubMed
