

Ictal high-frequency oscillations in neocortical epilepsy: implications for seizure localization and surgical resection
- PMID: 21762451
- PMCID: PMC3188690
- DOI: 10.1111/j.1528-1167.2011.03165.x
Ictal high-frequency oscillations in neocortical epilepsy: implications for seizure localization and surgical resection
Abstract
Purpose: To investigate the characteristics of intracranial ictal high-frequency oscillations (HFOs).
Methods: Among neocortical epilepsy patients who underwent intracranial monitoring and surgery, we studied patients with well-defined, unifocal seizure onsets characterized by discrete HFOs (≥70 Hz). Patients with multifocal or bilateral independent seizure onsets, electroencephalography (EEG) acquired at <1,000 Hz sampling rate, and nonresective surgery were excluded. Based on a prospectively defined protocol, we defined the seizure-onset zone (SOZ) presurgically to include only those channels with HFOs that showed subsequent sustained evolution (HFOs+ channels) but not the channels that lacked evolution (HFOs- channels). We then resected the SOZ as defined above, 1 cm of the surrounding cortex, and immediate spread area, modified by the presence of eloquent cortex in the vicinity. For purposes of this study, we also defined the SOZ based on the conventional frequency activity (CFA, <70 Hz) at seizure onset, although that information was not considered for preoperative determination of the surgical boundary. We investigated the temporal and spatial characteristics of the ictal HFOs post hoc by visual and spectral methods, and also compared them to the seizure onset defined by the CFA.
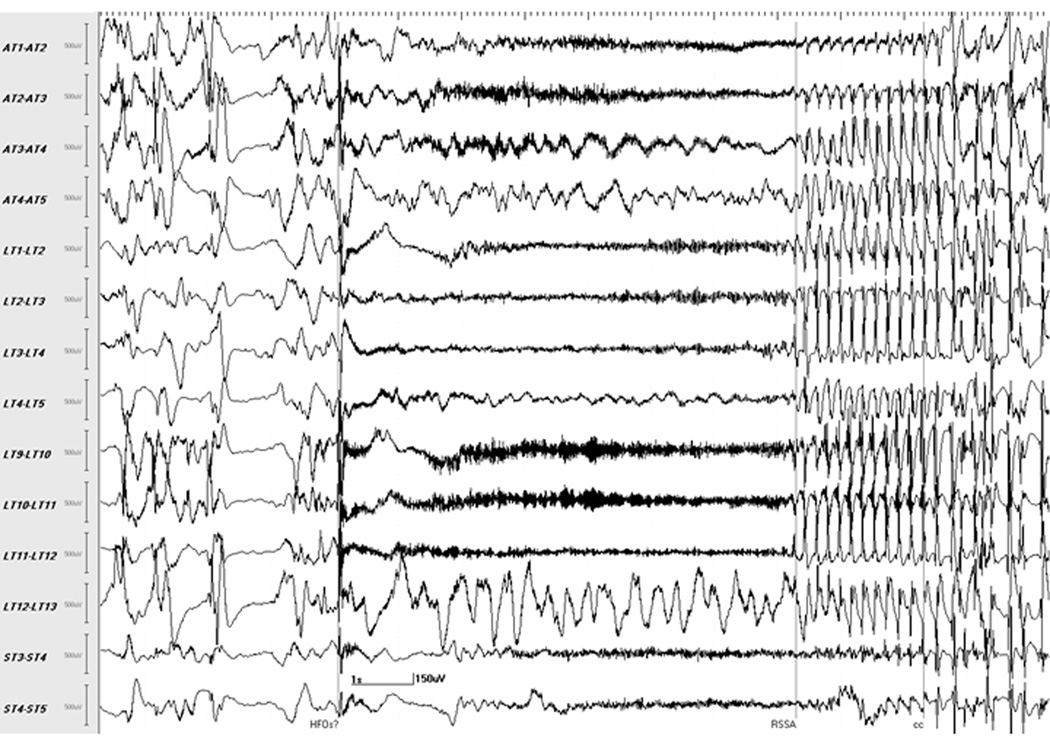
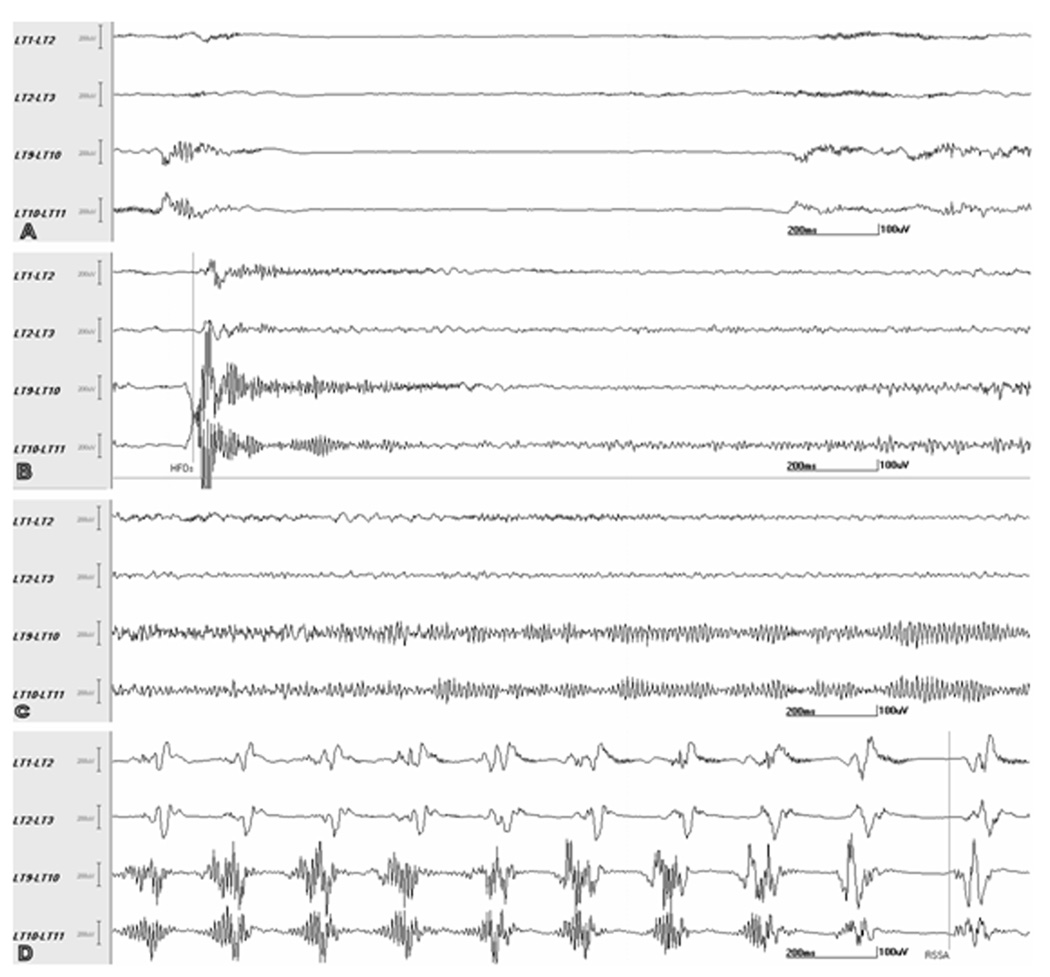
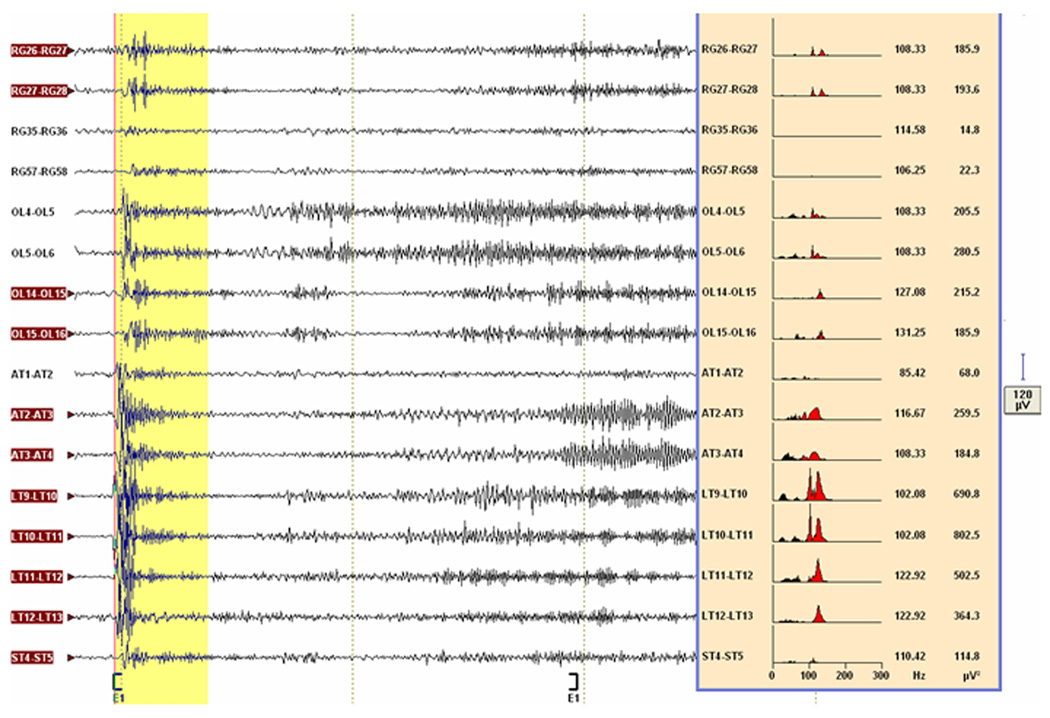
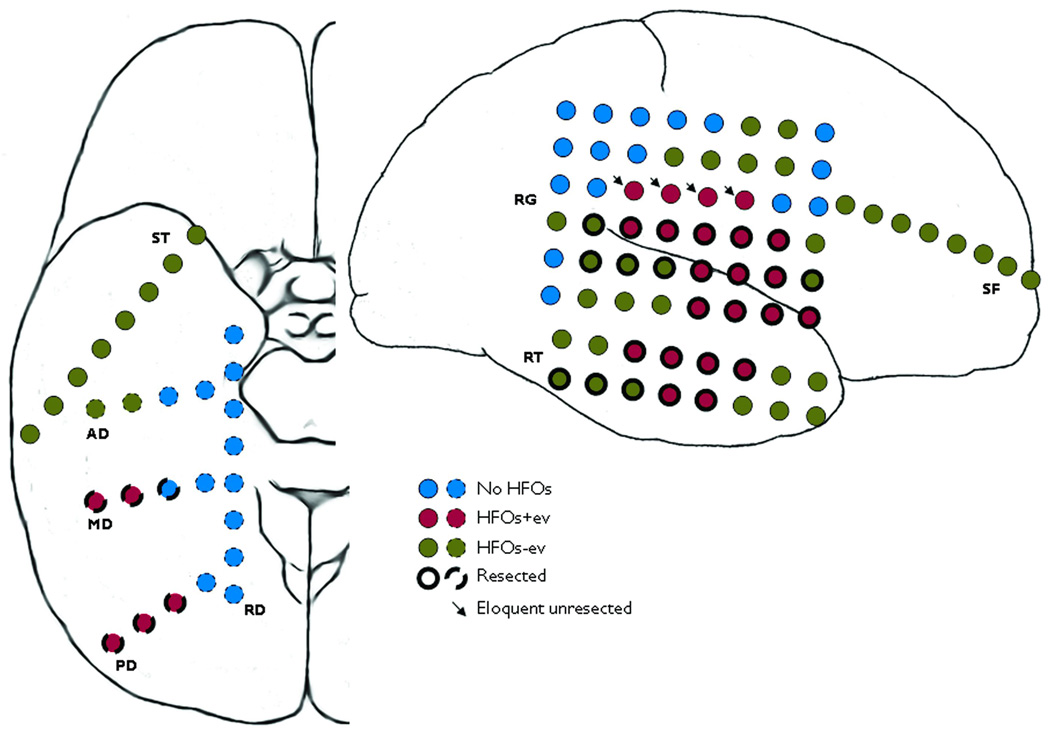
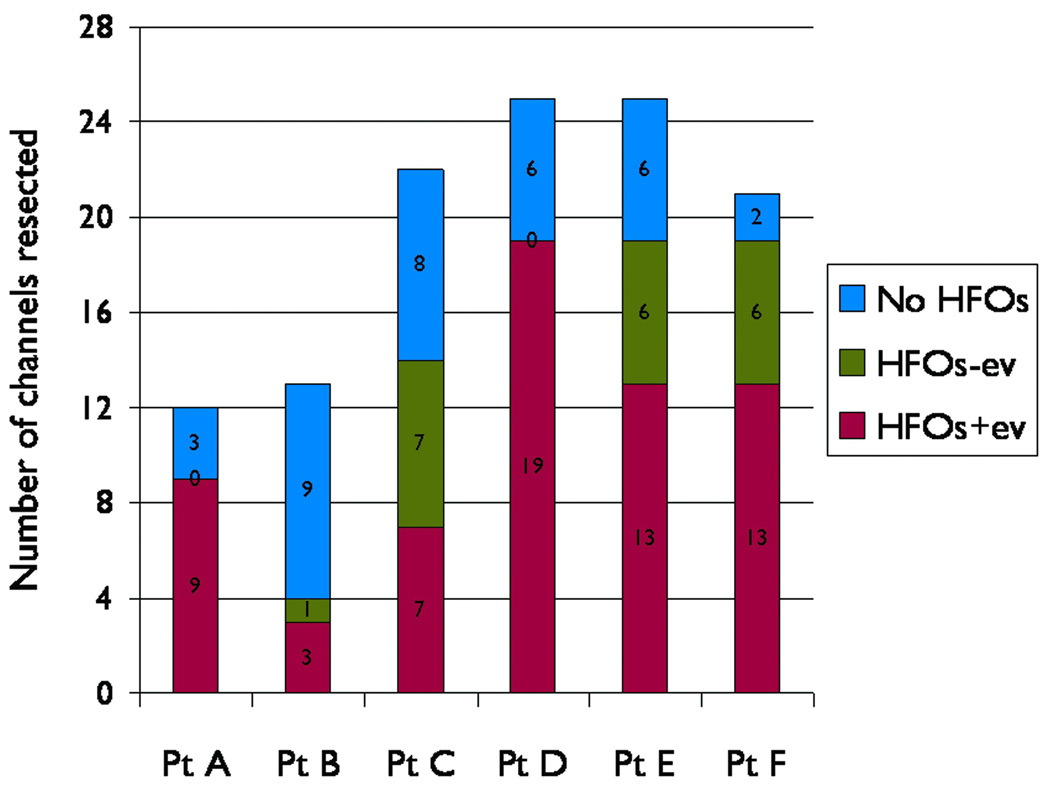
Key findings: Of 14 consecutive neocortical epilepsy patients, six patients met the inclusion criteria. Magnetic resonance imaging (MRI) was normal or showed heterotopia. All had subdural electrodes, with additional intracerebral depth electrodes in some. Electrode coverage was extensive (median 94 channels), including limited contralateral coverage. Seizure onsets were lobar or multilobar. Resections were performed per protocol, except in two patients where complete resection of the SOZ could not be done due to overlap with speech area. Histology was abnormal in all patients. Postoperative outcome was class I/II (n = 5, 83%) or class III over a mean follow-up of 27 months. Post hoc analysis of 15 representative seizures showed that the ictal HFOs were widespread at seizure onset but evolved subsequently with different characteristics. In contrast to HFOs-, the HFOs+ were significantly higher in peak frequency (97.1 vs. 89.1 Hz, p = 0.001), more robust (nearly twofold higher peak power, p < 0.0001), and spatially restricted [mean 12.2 vs. 22.4 channels; odds ratio (OR) 0.51, 95% confidence interval (CI) 0.42-0.62; p < 0.0001]. The seizure onset defined by HFOs+ was earlier (by an average of 0.41 s), and occurred in a significantly different and smaller distribution (OR 0.27, 95% CI 0.21-0.34, p < 0.0001), than the seizure onset defined by the CFA. As intended, the HFOs+ channels were 10 times more likely to have been resected than the HFOs- channels (OR 9.7, 95% CI 5-17, p < 0.0001).
Significance: Our study demonstrates the widespread occurrence of ictal HFOs at seizure onset, outlines a practical method to localize the SOZ based on their restricted pattern of evolution, and highlights the differences between the SOZs defined by HFOs and CFA. We show that smaller resections, restricted mainly to the HFOs channels with evolution, can lead to favorable seizure outcome. Our findings support the notion of widespread epileptic networks underlying neocortical epilepsy.
Wiley Periodicals, Inc. © 2011 International League Against Epilepsy.
Conflict of interest statement
None of the authors has any conflicts of interest to disclose.
Figures
Comment in
-
High-frequency oscillations pinpoint the seizure-onset zone.Nat Rev Neurol. 2011 Aug 23;7(9):475. doi: 10.1038/nrneurol.2011.127. Nat Rev Neurol. 2011. PMID: 21862988 No abstract available.
References
-
- Akiyama T, Otsubo H, Ochi A, Ishiguro T, Kadokura G, Ramachandrannair R, Weiss SK, Rutka JT, Carter Snead O., 3rd. Focal cortical high-frequency oscillations trigger epileptic spasms: confirmation by digital video subdural EEG. Clin Neurophysiol. 2005;116:2819–2825. - PubMed
-
- Alarcon G, Binnie CD, Elwes RD, Polkey CE. Power spectrum and intracranial EEG patterns at seizure onset in partial epilepsy. 1995;94:326–337. - PubMed
-
- Allen PJ, Fish DR, Smith SJ. Very high-frequency rhythmic activity during SEEG suppression in frontal lobe epilepsy. 1992;82:155–159. - PubMed
-
- Bragin A, Engel J, Jr, Wilson CL, Fried I, Buzsaki G. High-frequency oscillations in human brain. Hippocampus. 1999a;9:137–142. - PubMed
-
- Bragin A, Engel J, Jr, Wilson CL, Fried I, Mathern GW. Hippocampal and entorhinal cortex high-frequency oscillations (100--500 Hz) in human epileptic brain and in kainic acid--treated rats with chronic seizures. 1999b;40:127–137. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
