

C-reactive protein, an early marker of community-acquired sepsis resolution: a multi-center prospective observational study
- PMID: 21762483
- PMCID: PMC3387609
- DOI: 10.1186/cc10313
C-reactive protein, an early marker of community-acquired sepsis resolution: a multi-center prospective observational study
Abstract
Introduction: C-reactive protein (CRP) has been shown to be a valuable marker in the diagnosis of infection and in monitoring its response to antibiotics. Our objective was to evaluate serial CRP measurements after prescription of antibiotics to describe the clinical course of Community-Acquired Sepsis admitted to intensive care units (ICU).
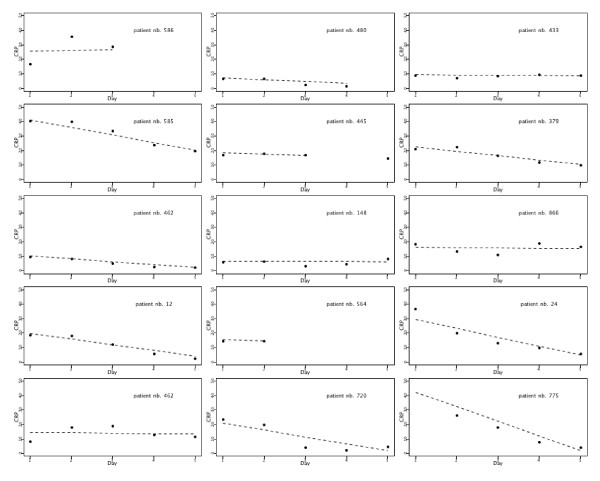
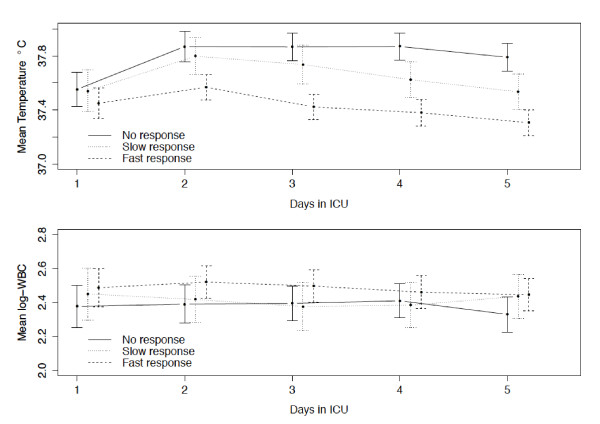
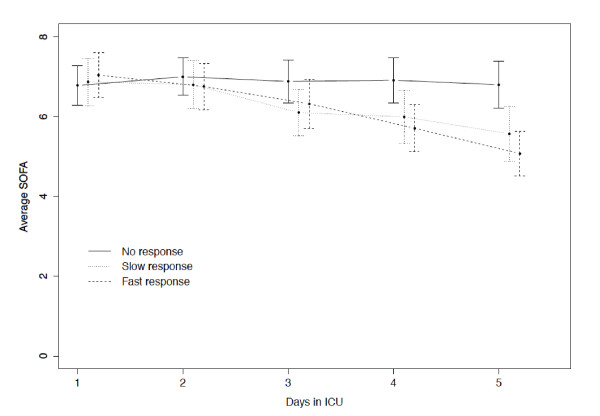
Methods: During a 12-month period a multi-center, prospective, observational study was conducted, segregating adults with Community-Acquired Sepsis. Patients were followed-up during the first five ICU days, day of ICU discharge or death and hospital outcome. CRP-ratio was calculated in relation to Day 1 CRP concentration. Patients were classified according to the pattern of CRP-ratio response to antibiotics: fast response if Day 5 CRP-ratio was < 0.4, slow response if Day 5 CRP-ratio was between 0.4 and 0.8, and no response if Day 5 CRP-ratio was > 0.8. Comparison between survivors and non-survivors was performed.
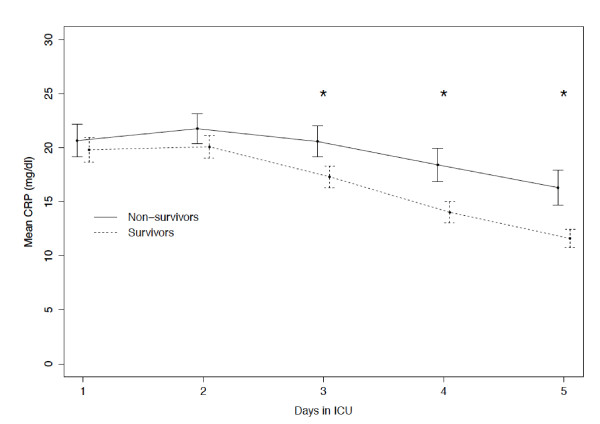
Results: A total of 891 patients (age 60 ± 17 yrs, hospital mortality 38%) were studied. There were no significant differences between the CRP of survivors and non-survivors until Day 2 of antibiotic therapy. On the following three days, CRP of survivors was significantly lower (P < 0.001). After adjusting for the Simplified Acute Physiology Score II and severity of sepsis, the CRP course was significantly associated with mortality (ORCRP-ratio = 1.03, confidence interval 95%= (1.02, 1.04), P < 0.001). The hospital mortality of patients with fast response, slow response and no response patterns was 23%, 30% and 41%, respectively (P = 0.001). No responders had a significant increase on the odds of death (OR = 2.5, CI95% = (1.6, 4.0), P < 0.001) when compared with fast responders.
Conclusions: Daily CRP measurements after antibiotic prescription were useful as early as Day 3 in identification of Community-Acquired Sepsis patients with poor outcome. The rate of CRP decline during the first five ICU days was markedly associated with prognosis. The identification of the pattern of CRP-ratio response was useful in the recognition of the individual clinical course.
Figures
Comment in
-
C-reactive protein in community-acquired sepsis: you can teach new tricks to an old dog.Crit Care. 2011;15(5):186. doi: 10.1186/cc10301. Epub 2011 Sep 7. Crit Care. 2011. PMID: 21955725 Free PMC article.
References
-
- Sprung CL, Sakr Y, Vincent JL, Le Gall JR, Reinhart K, Ranieri VM, Gerlach H, Fielden J, Groba CB, Payen D. An evaluation of systemic inflammatory response syndrome signs in the Sepsis Occurrence In Acutely Ill Patients (SOAP) study. Intensive Care Med. 2006;32:421–427. doi: 10.1007/s00134-005-0039-8. - DOI - PubMed
-
- Singh N, Rogers P, Atwood CW, Wagener MM, Yu VL. Short-course empiric antibiotic therapy for patients with pulmonary infiltrates in the intensive care unit. A proposed solution for indiscriminate antibiotic prescription. Am J Respir Crit Care Med. 2000;162:505–511. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
