

Localized reentry within the left atrial appendage: arrhythmogenic role in patients undergoing ablation of persistent atrial fibrillation
- PMID: 21762673
- PMCID: PMC3393101
- DOI: 10.1016/j.hrthm.2011.07.013
Localized reentry within the left atrial appendage: arrhythmogenic role in patients undergoing ablation of persistent atrial fibrillation
Abstract
Background: Left atrial appendage (LAA) is implicated in maintenance of atrial fibrillation (AF) and atrial tachycardia (AT) associated with persistent AF (PsAF) ablation, although little is known about the incidence and mechanism of LAA AT.
Objective: The purpose of this study was to characterize LAA ATs associated with PsAF ablation.
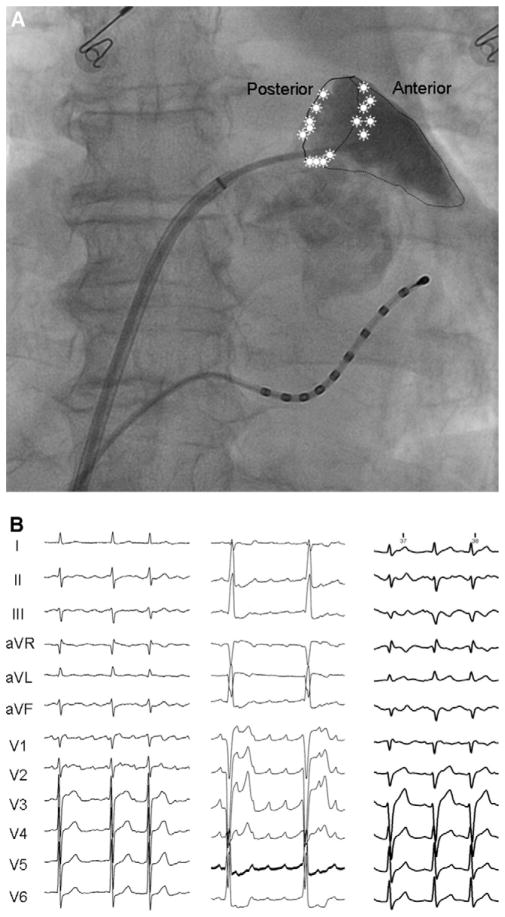
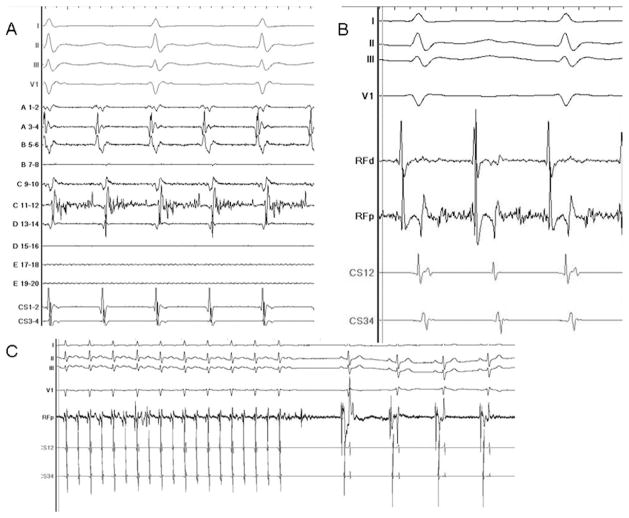
Methods: In 74 consecutive patients undergoing stepwise PsAF ablation, 142 ATs were encountered during index and repeat procedures. Out of 78 focal-source ATs diagnosed by activation and entrainment mapping, 15 (19%) arose from the base of LAA. Using a 20-pole catheter, high-density maps were constructed (n = 10; age 57 ± 6 years) to characterize the mechanism of LAA-AT. The LAA orifice was divided into the posterior ridge and anterior-superior and inferior segments to characterize the location of AT.
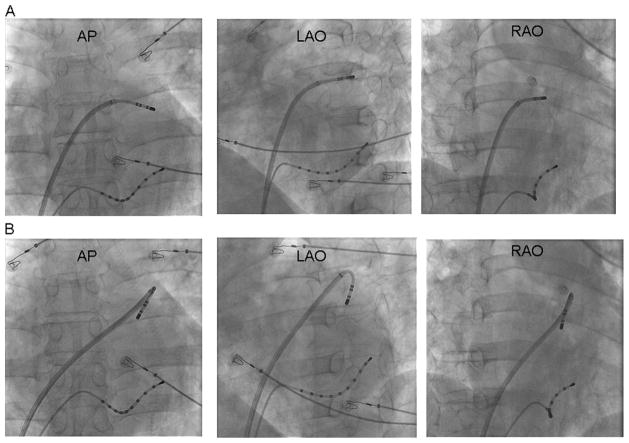
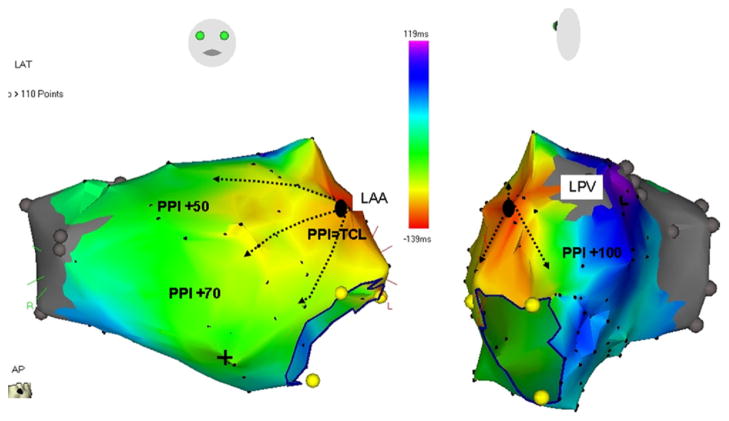
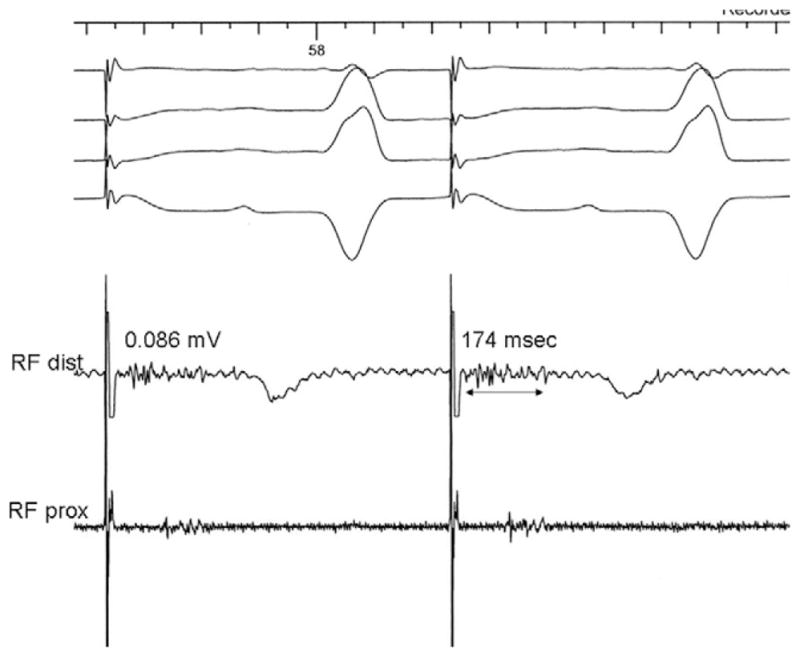
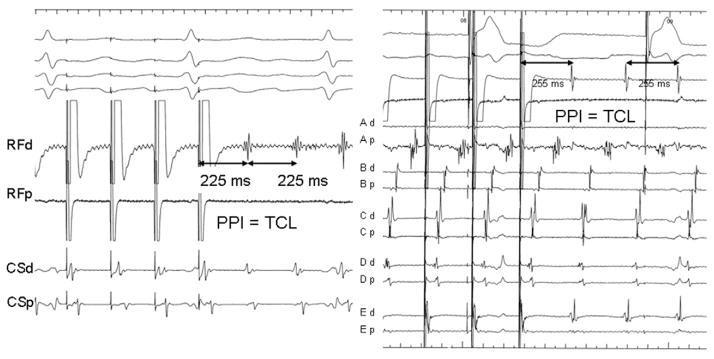
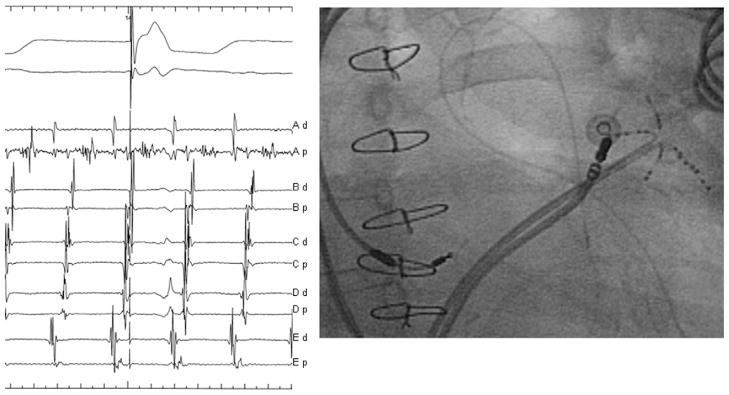
Results: Fifteen patients with LAA AT had symptomatic PsAF for 17 ± 15 months before ablation. LAA AT (cycle length [CL] 283 ± 30 ms) occurred during the index procedure in four and after 9 ± 7 months in 11 patients. We could map 89% ± 8% AT CLs locally with favorable entrainment from within the LAA, which is suggestive of localized reentry with centrifugal atrial activation. ATs were localized to inferior segment (n = 4), anterior-superior segment (n = 5), and posterior ridge (n = 6) with 1:1 conduction to the atria. Ablation targeting long fractionated or mid-diastolic electrogram within the LAA resulted in tachycardia termination. Postablation, selective contrast radiography demonstrated atrial synchronous LAA contraction in all but one patient. At 18 ± 7 months, 13/15 (87%) patients remained in sinus rhythm without antiarrhythmic drugs.
Conclusion: LAA is an important source of localized reentrant AT in patients with PsAF at index and repeat ablation procedures. Ablation targeting the site with long fractionated or mid-diastolic LAA electrogram is highly effective in acute and medium-term elimination of the arrhythmia.
Copyright © 2011. Published by Elsevier Inc.
Figures
References
-
- Di Biase L, Burkhardt JD, Mohanty P, et al. Left atrial appendage: an under-recognized trigger site of atrial fibrillation. Circulation. 2010;122:109–118. - PubMed
-
- Haïssaguerre M, Hocini M, Sanders P, et al. Localized sources maintaining atrial fibrillation organized by prior ablation. Circulation. 2006;113:616– 625. - PubMed
-
- Haïssaguerre M, Sanders P, Hocini M, et al. Catheter ablation of long-lasting persistent atrial fibrillation: critical structures for termination. J Cardiovasc Electrophysiol. 2005;16:1125–1137. - PubMed
-
- Kato M, Adachi M, Yano A, et al. Radiofrequency catheter ablation for atrial tachycardia originating from the left atrial appendage. J Interv Card Electrophysiol. 2007;19:45– 48. - PubMed
-
- Kistler PM, Roberts-Thomson KC, Haqqani HM, et al. P-wave morphology in focal atrial tachycardia: development of an algorithm to predict the anatomic site of origin. J Am Coll Cardiol. 2006;48:1010–1017. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
