

3D virtual human atria: A computational platform for studying clinical atrial fibrillation
- PMID: 21762716
- PMCID: PMC3211061
- DOI: 10.1016/j.pbiomolbio.2011.06.011
3D virtual human atria: A computational platform for studying clinical atrial fibrillation
Abstract
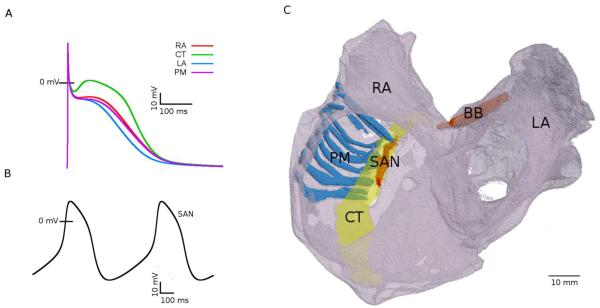
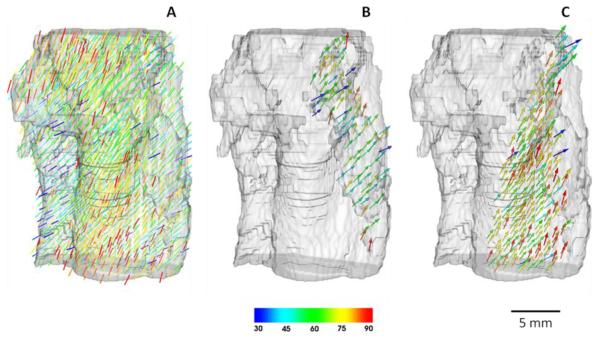
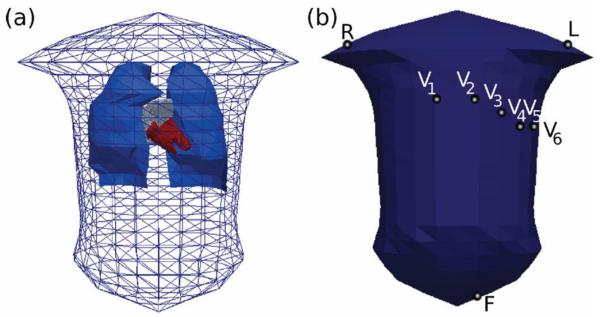
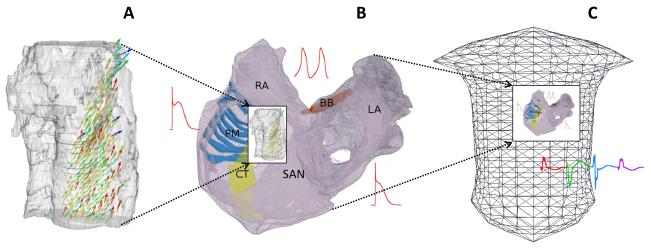
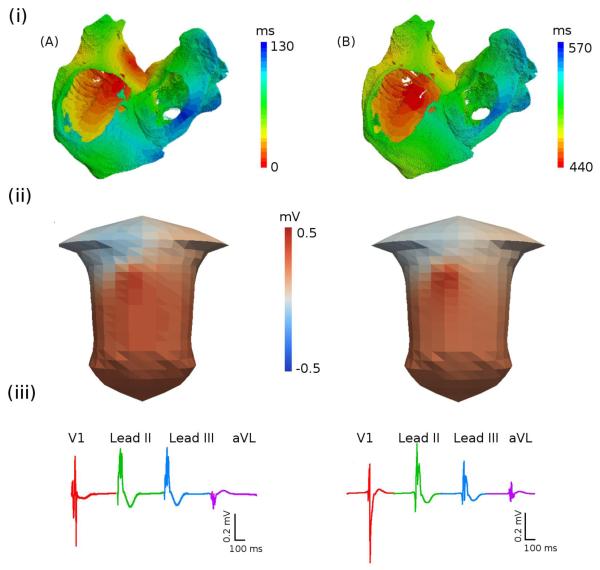
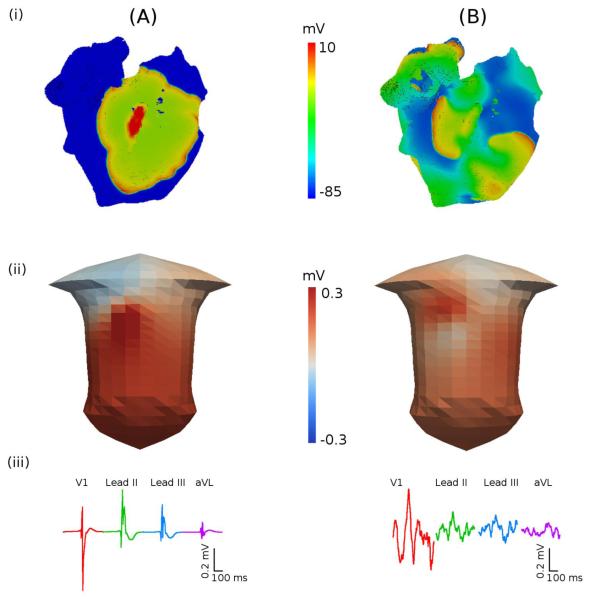
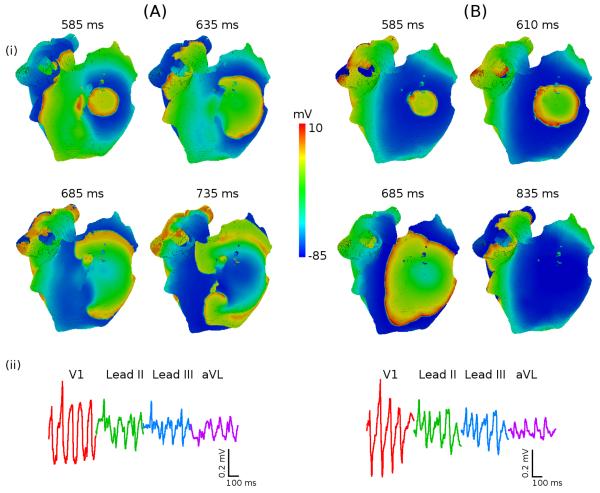
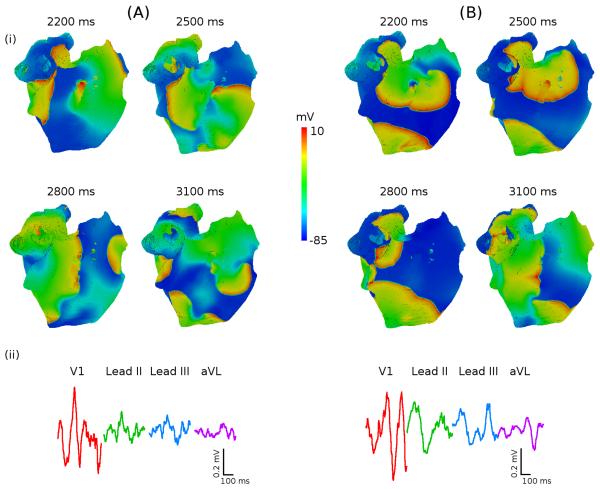
Despite a vast amount of experimental and clinical data on the underlying ionic, cellular and tissue substrates, the mechanisms of common atrial arrhythmias (such as atrial fibrillation, AF) arising from the functional interactions at the whole atria level remain unclear. Computational modelling provides a quantitative framework for integrating such multi-scale data and understanding the arrhythmogenic behaviour that emerges from the collective spatio-temporal dynamics in all parts of the heart. In this study, we have developed a multi-scale hierarchy of biophysically detailed computational models for the human atria--the 3D virtual human atria. Primarily, diffusion tensor MRI reconstruction of the tissue geometry and fibre orientation in the human sinoatrial node (SAN) and surrounding atrial muscle was integrated into the 3D model of the whole atria dissected from the Visible Human dataset. The anatomical models were combined with the heterogeneous atrial action potential (AP) models, and used to simulate the AP conduction in the human atria under various conditions: SAN pacemaking and atrial activation in the normal rhythm, break-down of regular AP wave-fronts during rapid atrial pacing, and the genesis of multiple re-entrant wavelets characteristic of AF. Contributions of different properties of the tissue to mechanisms of the normal rhythm and arrhythmogenesis were investigated. Primarily, the simulations showed that tissue heterogeneity caused the break-down of the normal AP wave-fronts at rapid pacing rates, which initiated a pair of re-entrant spiral waves; and tissue anisotropy resulted in a further break-down of the spiral waves into multiple meandering wavelets characteristic of AF. The 3D virtual atria model itself was incorporated into the torso model to simulate the body surface ECG patterns in the normal and arrhythmic conditions. Therefore, a state-of-the-art computational platform has been developed, which can be used for studying multi-scale electrical phenomena during atrial conduction and AF arrhythmogenesis. Results of such simulations can be directly compared with electrophysiological and endocardial mapping data, as well as clinical ECG recordings. The virtual human atria can provide in-depth insights into 3D excitation propagation processes within atrial walls of a whole heart in vivo, which is beyond the current technical capabilities of experimental or clinical set-ups.
Copyright © 2011 Elsevier Ltd. All rights reserved.
Figures
References
-
- Allessie MA, Bonke FI, Schopmann FTG. Circus movement in rabbit atrial muscle as a mechanism of tachycardia. II. The role of nonuniform recovery of excitability in the occurrence of unidirectional block studied with multiple microelectrodes. Circ Res. 1976;39:168–77. - PubMed
-
- Anter E, Jessup M, Callans DJ. Atrial fibrillation and heart failure: treatment considerations for a dual epidemic. Circulation. 2009;119:2516–25. - PubMed
-
- Basser PJ, Mattiello J, LeBihan D. Estimation of the effective self-diffusion tensor from the NMR spin echo. J Magnet Res Med. 1994;30:201–206. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
