

Myocardial remodeling with aortic stenosis and after aortic valve replacement: mechanisms and future prognostic implications
- PMID: 21762938
- PMCID: PMC3210937
- DOI: 10.1016/j.jtcvs.2011.04.044
Myocardial remodeling with aortic stenosis and after aortic valve replacement: mechanisms and future prognostic implications
Abstract
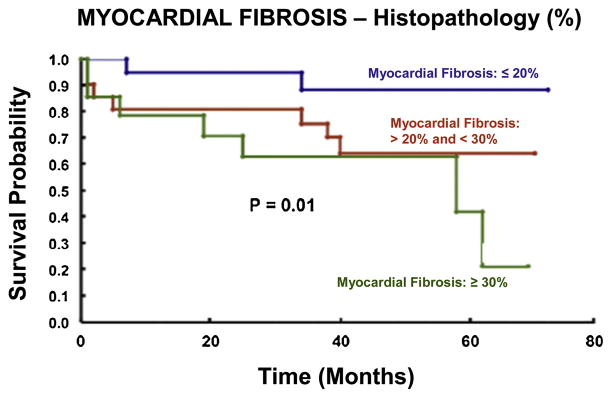
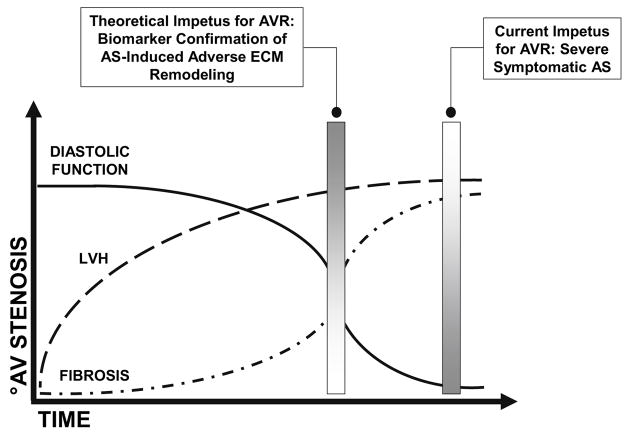
Aortic valve stenosis is a common cause of left ventricular pressure overload, a pathologic process that elicits myocyte hypertrophy and alterations in extracellular matrix composition, both of which contribute to increases in left ventricular stiffness. However, clinical and animal studies suggest that increased myocardial extracellular matrix fibrillar collagen content occurs later in the time course of left ventricular pressure overload at a time coincident with severe abnormalities in diastolic function followed by the development of symptomatic heart failure. Aortic valve replacement remains the most effective treatment for elimination of chronic pressure overload secondary to aortic stenosis but has traditionally been recommended only after the onset of clinical symptoms. Long-term follow-up of patients with symptomatic aortic stenosis after aortic valve replacement suggests that valve replacement may not result in complete reversal of the maladaptive changes that occur within the myocardial extracellular matrix secondary to the pressure overload state. To the contrary, residual left ventricular extracellular matrix abnormalities such as these are likely responsible for persistent abnormalities in diastolic function and increased morbidity and mortality after aortic valve replacement. Defining the mechanisms and pathways responsible for regulating the myocardial extracellular matrix during the natural history of aortic stenosis may provide a means by which to detect crucial structural milestones and thereby permit more precise identification of the development of maladaptive left ventricular remodeling.
Published by Mosby, Inc.
Figures

References
-
- Badeer HS. Biological significance of cardiac hypertrophy. Am J Cardiol. 1964;14:133–138. - PubMed
-
- Alpert NR. Cardiac hypertrophy. Academic Press, Inc; New York: 1971. Preface; pp. XV–XVI.
-
- Carabello BA, Paulus WJ. Aortic Stenosis. Lancet. 2009;373:956–66. - PubMed
-
- Monrad ES, Hess OM, Murakami T, et al. Time course of regression of left ventricular hypertrophy after aortic valve replacement. Circulation. 1988;77(6):1345–55. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
