

The impact of increased chest compression fraction on return of spontaneous circulation for out-of-hospital cardiac arrest patients not in ventricular fibrillation
- PMID: 21763252
- PMCID: PMC3215827
- DOI: 10.1016/j.resuscitation.2011.07.011
The impact of increased chest compression fraction on return of spontaneous circulation for out-of-hospital cardiac arrest patients not in ventricular fibrillation
Abstract
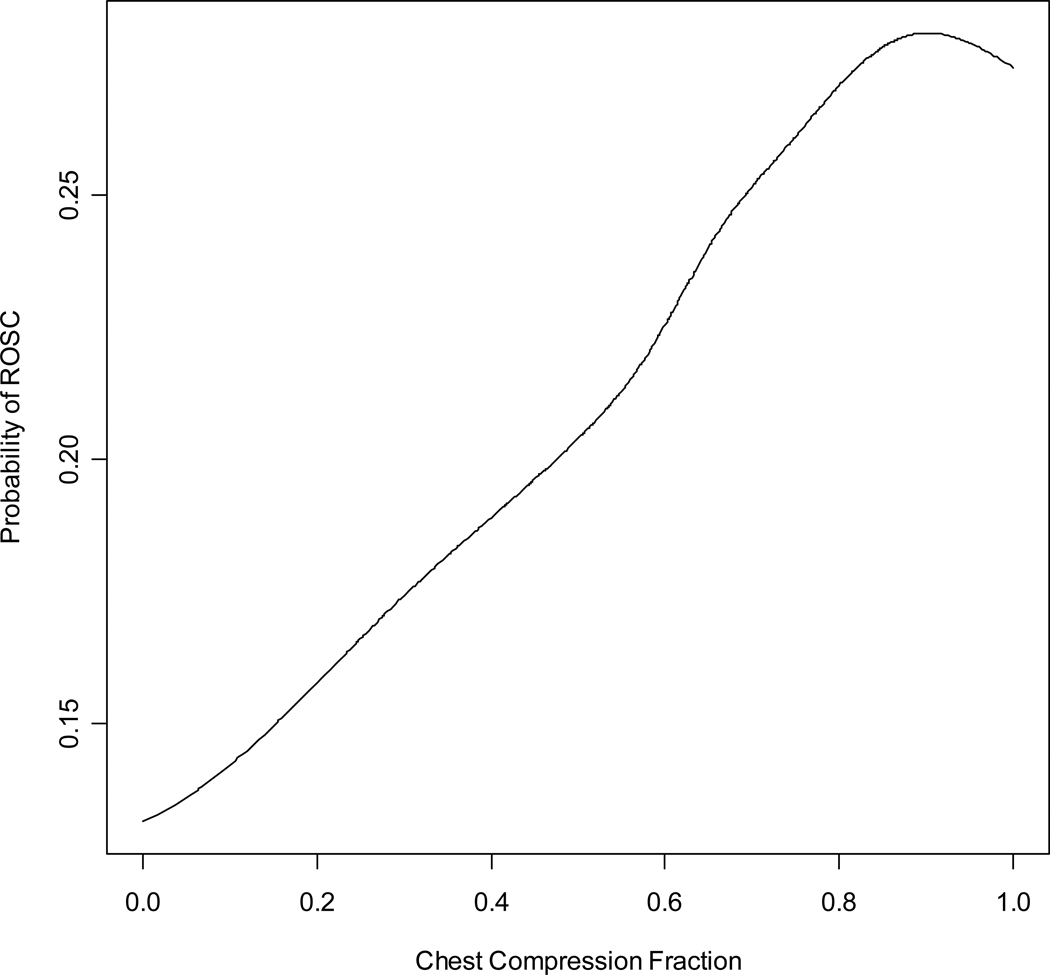
Objective: Greater chest compression fraction (CCF, or proportion of CPR time spent providing compressions) is associated with better survival for out-of-hospital cardiac arrest (OOHCA) patients in ventricular fibrillation (VF). We evaluated the effect of CCF on return of spontaneous circulation (ROSC) in OOHCA patients with non-VF ECG rhythms in the Resuscitation Outcomes Consortium Epistry.
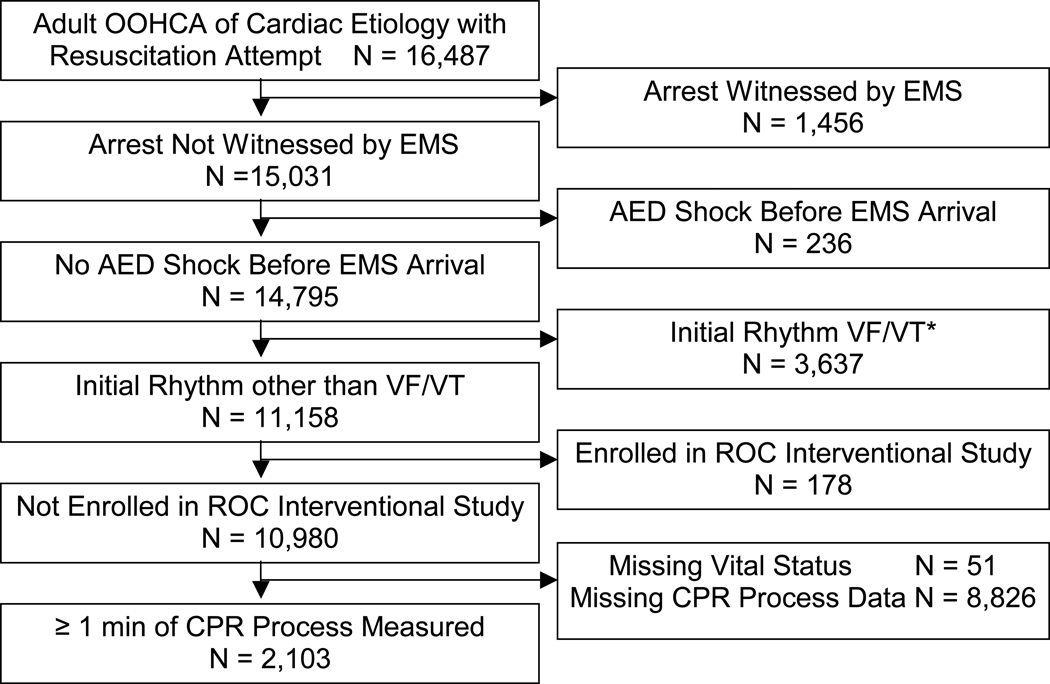
Methods: This prospective cohort study included OOHCA patients if: not witnessed by EMS, no automated external defibrillator (AED) shock prior to EMS arrival, received >1 min of CPR with CPR process measures available, and initial non-VF rhythm. We reviewed the first 5 min of electronic CPR records following defibrillator application, measuring the proportion of compressions/min during the resuscitation.
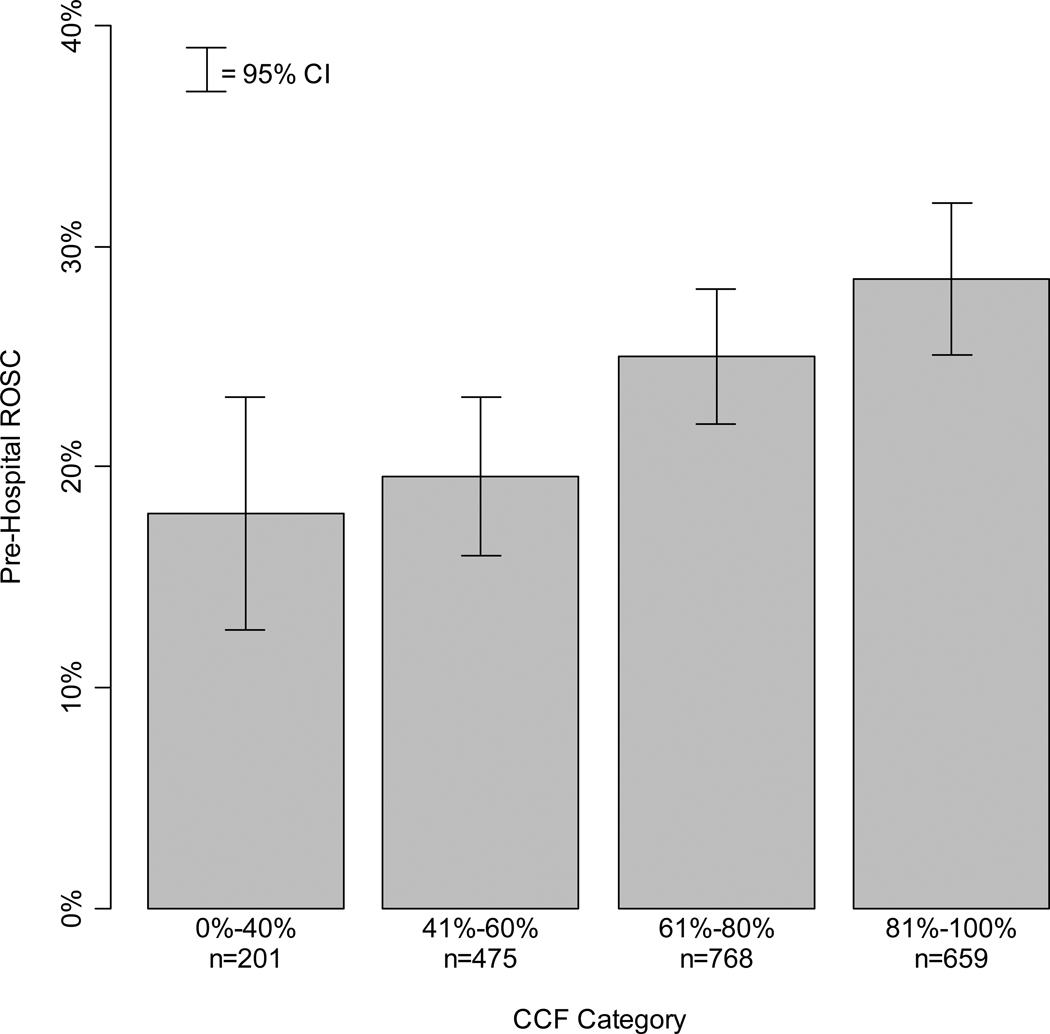
Results: Demographics of 2103 adult patients from 10 U.S. and Canadian centers were: mean age 67.8; male 61.2%; public location 10.6%; bystander witnessed 32.9%; bystander CPR 35.4%; median interval from 911 to defibrillator turned on 8 min:27 s; initial rhythm asystole 64.0%, PEA 28.0%, other non-shockable 8.0%; median compression rate 110/min; median CCF 71%; ROSC 24.2%; survival to hospital discharge 2.0%. The estimated linear effect on adjusted odds ratio with 95% confidence interval (OR; 95%CI) of ROSC for each 10% increase in CCF was (1.05; 0.99, 1.12). Adjusted (OR; 95%CI) of ROSC for each CCF category were: 0-40% (reference group); 41-60% (1.14; 0.72, 1.81); 61-80% (1.42; 0.92, 2.20); and 81-100% (1.48; 0.94, 2.32).
Conclusions: This is the first study to demonstrate that increased CCF among non-VF OOHCA patients is associated with a trend toward increased likelihood of ROSC.
Copyright © 2011 Elsevier Ireland Ltd. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
During CPR, push hard and fast and please do not stop!Resuscitation. 2011 Dec;82(12):1475-6. doi: 10.1016/j.resuscitation.2011.08.026. Epub 2011 Sep 17. Resuscitation. 2011. PMID: 21930106 No abstract available.
References
-
- Vaillancourt C, Stiell IG. Canadian Cardiovascular Outcomes Research Team (CCORT). Cardiac arrest care and emergency medical services in Canada. Canadian Journal of Cardiology. 2004;20(11):1081–1090. - PubMed
-
- Stiell IG, Wells GA, Field B, et al. Advanced cardiac life support in out-of-hospital cardiac arrest. New England Journal of Medicine. 2004;351(7):647–656. - PubMed
-
- Abella BS, Edelson DP, Kim S, et al. CPR quality improvement during in-hospital cardiac arrest using a real-time audiovisual feedback system. Resuscitation. 2007 Apr;73(1):54–61. - PubMed
-
- Edelson DP, Abella BS, Kramer-Johansen J, et al. Effects of compression depth and pre-shock pauses predict defibrillation failure during cardiac arrest. Resuscitation. 2006 Nov;71(2):137–145. - PubMed
Publication types
MeSH terms
Grants and funding
- 1RC2HL101759-01/HL/NHLBI NIH HHS/United States
- U01 HL077866/HL/NHLBI NIH HHS/United States
- R01 HL089554-03/HL/NHLBI NIH HHS/United States
- HL077867/HL/NHLBI NIH HHS/United States
- 5U01 HL077863/HL/NHLBI NIH HHS/United States
- HL077887/HL/NHLBI NIH HHS/United States
- U01 HL077881/HL/NHLBI NIH HHS/United States
- HL077873/HL/NHLBI NIH HHS/United States
- HL077871/HL/NHLBI NIH HHS/United States
- HL077881/HL/NHLBI NIH HHS/United States
- HL077908/HL/NHLBI NIH HHS/United States
- U01 HL077863-05/HL/NHLBI NIH HHS/United States
- U01 HL077871/HL/NHLBI NIH HHS/United States
- U01 HL077887/HL/NHLBI NIH HHS/United States
- U01 HL077885/HL/NHLBI NIH HHS/United States
- CAPMC/ CIHR/Canada
- U01 HL077865/HL/NHLBI NIH HHS/United States
- U01 HL077863/HL/NHLBI NIH HHS/United States
- U01 HL077908/HL/NHLBI NIH HHS/United States
- HL077872/HL/NHLBI NIH HHS/United States
- HL077866/HL/NHLBI NIH HHS/United States
- U01 HL077873/HL/NHLBI NIH HHS/United States
- R21 HL093641-01A1/HL/NHLBI NIH HHS/United States
- U01 HL077867/HL/NHLBI NIH HHS/United States
- HL077885/HL/NHLBI NIH HHS/United States
- HL077865/HL/NHLBI NIH HHS/United States
- U01 HL077872/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
