

Local and systemic alterations in signal transducers and activators of transcription (STAT) associated with human abdominal aortic aneurysms
- PMID: 21764069
- PMCID: PMC3197955
- DOI: 10.1016/j.jss.2011.05.041
Local and systemic alterations in signal transducers and activators of transcription (STAT) associated with human abdominal aortic aneurysms
Abstract
Background: Signal transducers and activators of transcription (STAT) proteins are transcription factors that, when activated by phosphorylation, regulate gene expression and cellular activity. The aim of this study was to evaluate the local and systemic expression and activation of STAT proteins associated with abdominal aortic aneurysms (AAA).
Methods: Expression and activation of STAT proteins were assessed in aortic wall samples obtained from patients undergoing repair of AAA (n = 9) and from non-aneurysmal (NA) donors (n = 17). Aortic samples were evaluated for mRNA and protein expression for STAT1, 2, 3, 4, 5a, and 5b using RT-PCR and immunoblot (WB) assays and normalized to ß-actin (expressed as arbitrary units). STAT activation was assessed with WB assays using phosphorylated (p)-STAT-specific antibodies. Alterations in STAT activation were calculated by normalizing pSTAT proteins to corresponding total STAT levels. Immunohistochemistry was performed on AAA and NA samples using the total and pSTAT antibodies. Systemic alterations in STAT activation were assessed by evaluating circulating leukocytes for the presence of pSTAT from patients with AAA (AAA, n = 8), repaired aneurysm (RA, n = 8), or age/gender matched controls with no AAA (CT, n = 8). Flow cytometry was performed to assess for circulating levels of STAT1 (pY701), STAT3 (pY705), and STAT5a (pY694) in monocytes, granulocytes, and lymphocytes. Assessments were made at baseline and in response to in vitro stimulation with IFN-γ (50 ng/mL) or IL-6 (100 ng/mL). Results were analyzed using Student's t-test and are expressed as mean ± SEM.
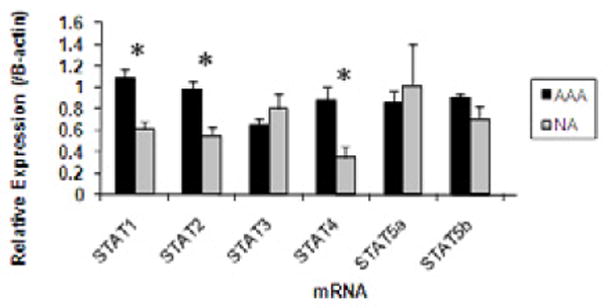
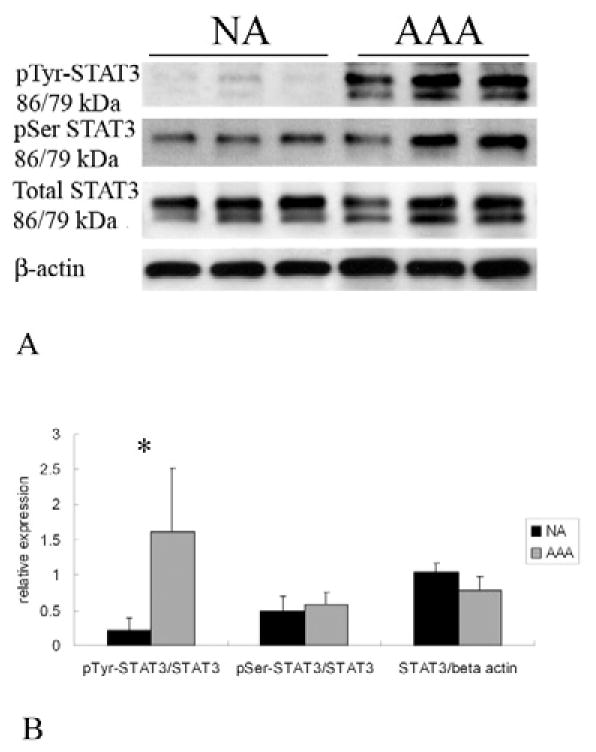
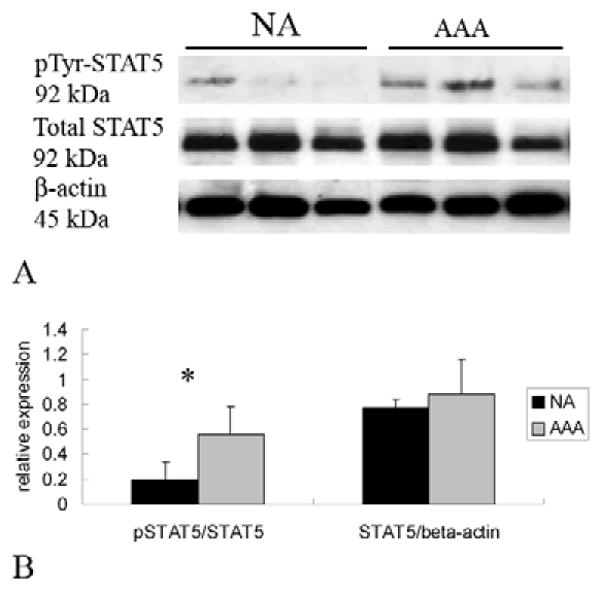
Results: In AAA tissue compared with NA, STAT-1 (1.08 ± 0.09 versus 0.62 ± 0.07), -2 (0.98 ± 0.07 versus 0.55 ± 0.08), and -4 (0.89 ± 0.12 versus 0.35 ± 0.11) mRNA levels were elevated (P < 0.01, all). Corresponding increases in STAT protein were only observed for STAT1 (2.77 ± 0.93 versus 0.93 ± 0.08, P < 0.05). Increases in activation were observed in AAA compared with NA in pSTAT2 (0.77 ± 0.1 versus 0.1 ± 0.02, P < 0.01), pSTAT3 (1.6 ± 0.3 versus 0.2 ± 0.06, P < 0.02) and pSTAT5 (0.57 ± 0.03 versus 0.2 ± 0.03, P < 0.05) levels. Phosphorylated STAT1, 2, 3, and 5 were observed in inflammatory cells invading the AAA adventitia. In addition, STAT3 was observed in the media of AAA and NA, but pSTAT3 was only observed in the media of AAA. There were no differences in baseline levels of pSTAT-positive circulating leukocytes. IFN-γ stimulation decreased STAT-5a (pY694)-positive CT lymphocytes to 40% ± 13% of baseline, but had no effect on AAA or RA lymphocytes (116% ± 35%, 102% ± 19%, respectively; P = 0.01). STAT-5a (pY694)-positive CT granulocytes also decreased to 62% ± 18% of baseline compared with AAA or RA granulocytes (122% ± 25%, 126% ± 17%, respectively; P = 0.01). Alterations in STAT1 (pY701) and STAT3 (pY705) were not observed in leukocytes following cytokine stimulation.
Conclusions: STAT proteins are important regulators of transcriptional activity and have been linked to cardiovascular disease. The present data suggest that altered levels of phosphorylated STATs are associated with AAA. Understanding their role may provide further insight into the mechanisms of AAA formation and allow for the development of medical treatment options.
Copyright © 2012 Elsevier Inc. All rights reserved.
Figures





References
-
- Saratzis A, Kitas GD, Saratzis N, Melas N. Can statins suppress the development of abdominal aortic aneurysms? A review of the current evidence. Angiology. 2010;61:137–44. - PubMed
-
- Shimizu K, Mitchell RN, Libby P. Inflammation and cellular immune responses in abdominal aortic aneurysms. Arterioscler Thromb Vasc Biol. 2006;26(5):987–94. - PubMed
-
- Ocana E, Perez-Requena J, Bohorquez J, Brieva J, Rodriguez C. Chemokine receptor expression on infiltrating lymphocytes from abdominal aortic aneurysms: role of CXCR4-CXCL12 in lymphoid recruitment. Atherosclerosis. 2008;200:264–70. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
