

Accuracy of the Xpert MTB/RIF test for the diagnosis of pulmonary tuberculosis in children admitted to hospital in Cape Town, South Africa: a descriptive study
- PMID: 21764384
- PMCID: PMC4202386
- DOI: 10.1016/S1473-3099(11)70167-0
Accuracy of the Xpert MTB/RIF test for the diagnosis of pulmonary tuberculosis in children admitted to hospital in Cape Town, South Africa: a descriptive study
Abstract
Background: WHO recommends that Xpert MTB/RIF replaces smear microscopy for initial diagnosis of suspected HIV-associated tuberculosis or multidrug-resistant pulmonary tuberculosis, but no data exist for its use in children. We aimed to assess the accuracy of the test for the diagnosis of pulmonary tuberculosis in children in an area with high tuberculosis and HIV prevalences.
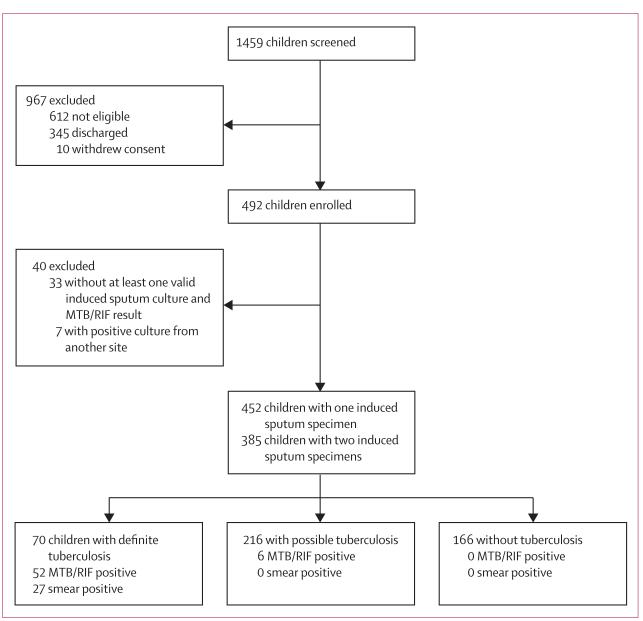
Methods: In this prospective, descriptive study, we enrolled children aged 15 years or younger who had been admitted to one of two hospitals in Cape Town, South Africa, with suspected pulmonary tuberculosis between Feb 19, 2009, and Nov 30, 2010. We compared the diagnostic accuracy of MTB/RIF and concentrated, fluorescent acid-fast smear with a reference standard of liquid culture from two sequential induced sputum specimens (primary analysis).
Results: 452 children (median age 19·4 months, IQR 11·1-46·2) had at least one induced sputum specimen; 108 children (24%) had HIV infection. 27 children (6%) had a positive smear result, 70 (16%) had a positive culture result, and 58 (13%) had a positive MTB/RIF test result. With mycobacterial culture as the reference standard, MTB/RIF tests when done on two induced sputum samples detected twice as many cases (75·9%, 95% CI 64·5-87·2) as did smear microscopy (37·9%, 25·1-50·8), detecting all of 22 smear-positive cases and 22 of 36 (61·1%, 44·4-77·8) smear-negative cases. For smear-negative cases, the incremental increase in sensitivity from testing a second specimen was 27·8% for MTB/RIF, compared with 13·8% for culture. The specificity of MTB/RIF was 98·8% (97·6-99·9). MTB/RIF results were available in median 1 day (IQR 0-4) compared with median 12 days (9-17) for culture (p<0·0001).
Interpretation: MTB/RIF testing of two induced sputum specimens is warranted as the first-line diagnostic test for children with suspected pulmonary tuberculosis.
Funding: National Institutes of Health, the National Health Laboratory Service Research Trust, the Medical Research Council of South Africa, and Wellcome Trust.
Copyright © 2011 Elsevier Ltd. All rights reserved.
Comment in
-
New research and development strategy for tuberculosis diagnostics urgently needed.Lancet Infect Dis. 2012 Aug;12(8):584-5. doi: 10.1016/S1473-3099(12)70166-4. Lancet Infect Dis. 2012. PMID: 22835891 No abstract available.
References
-
- Zar HJ, Connell TG, Nicol M. Diagnosis of pulmonary tuberculosis in children: new advances. Expert Rev Anti Infect Ther. 2010;8:277–88. - PubMed
-
- Hesseling AC, Schaaf HS, Gie RP, Starke JR, Beyers N. A critical review of diagnostic approaches used in the diagnosis of childhood tuberculosis. Int J Tuberc Lung Dis. 2002;6:1038–45. - PubMed
-
- Zar HJ, Hanslo D, Apolles P, Swingler G, Hussey G. Induced sputum versus gastric lavage for microbiological confirmation of pulmonary tuberculosis in infants and young children: a prospective study. Lancet. 2005;365:130–34. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
