

Vitamin A deficiency impairs vaccine-elicited gastrointestinal immunity
- PMID: 21765014
- PMCID: PMC3150351
- DOI: 10.4049/jimmunol.1101248
Vitamin A deficiency impairs vaccine-elicited gastrointestinal immunity
Abstract
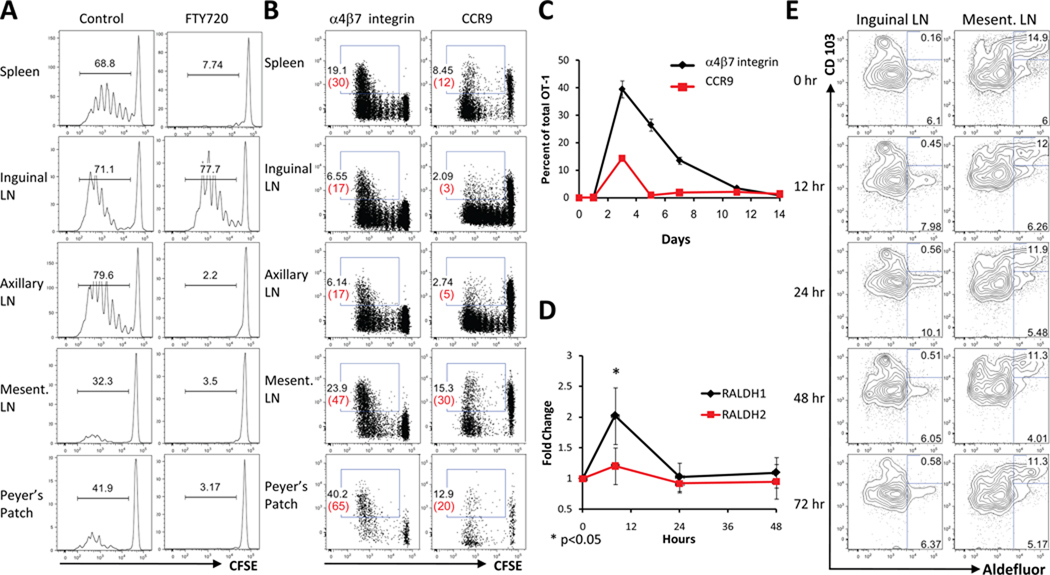
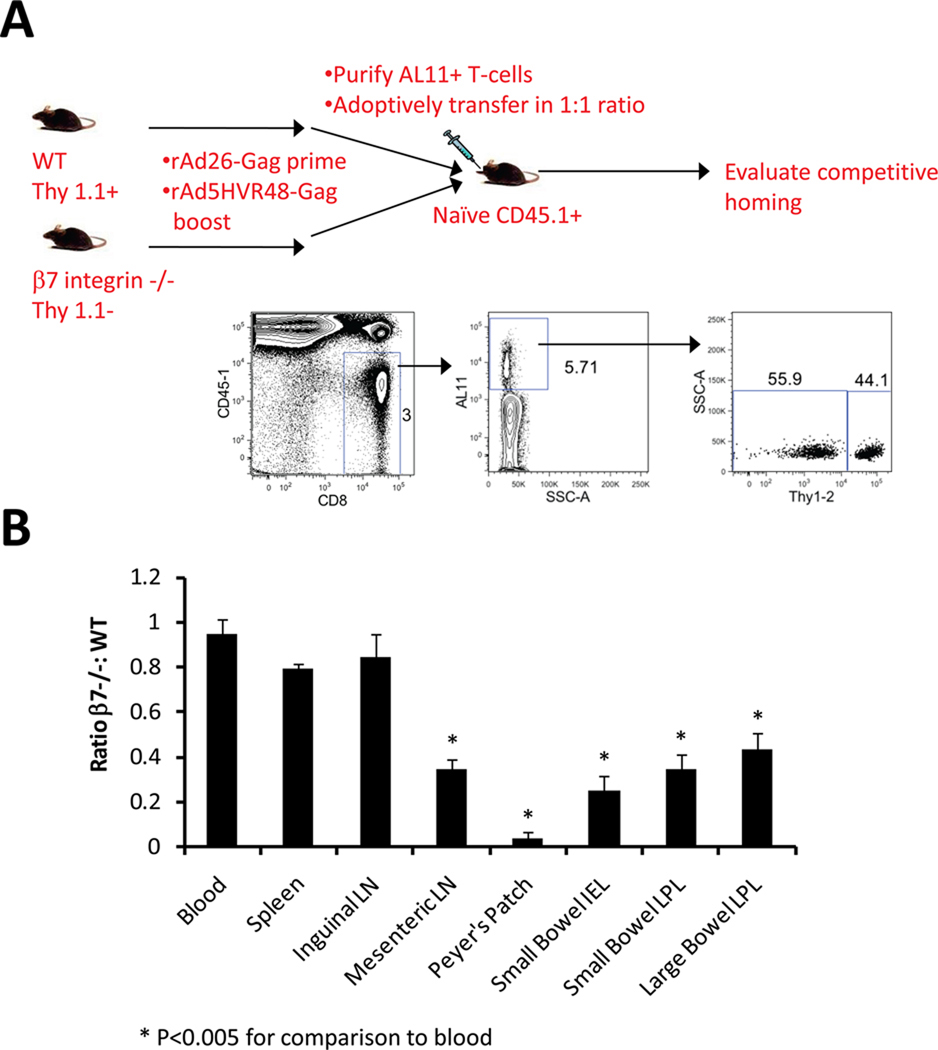
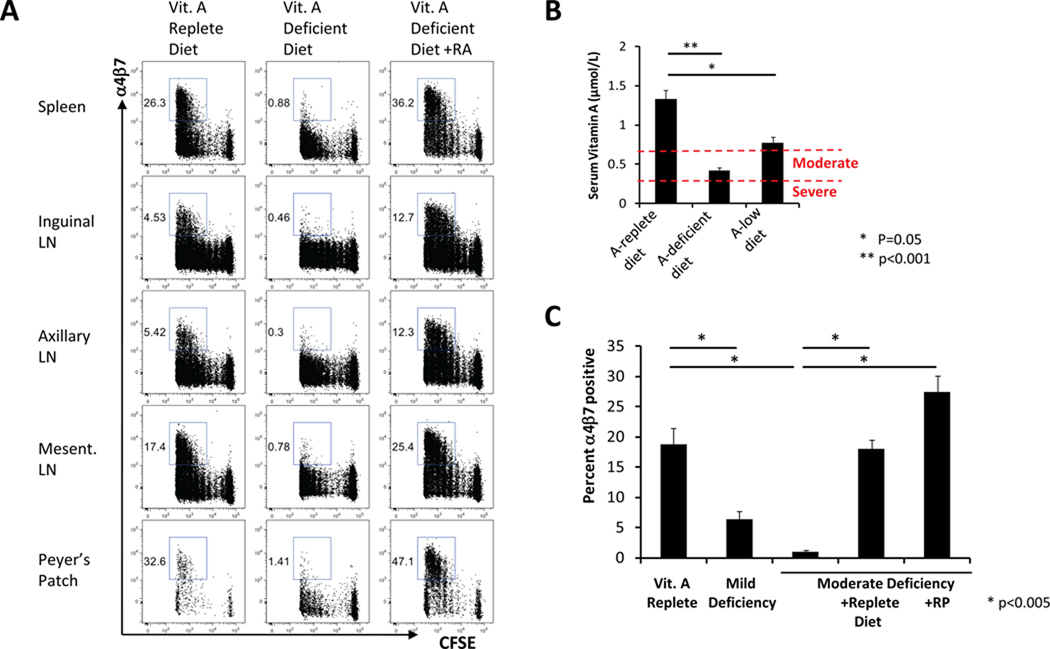
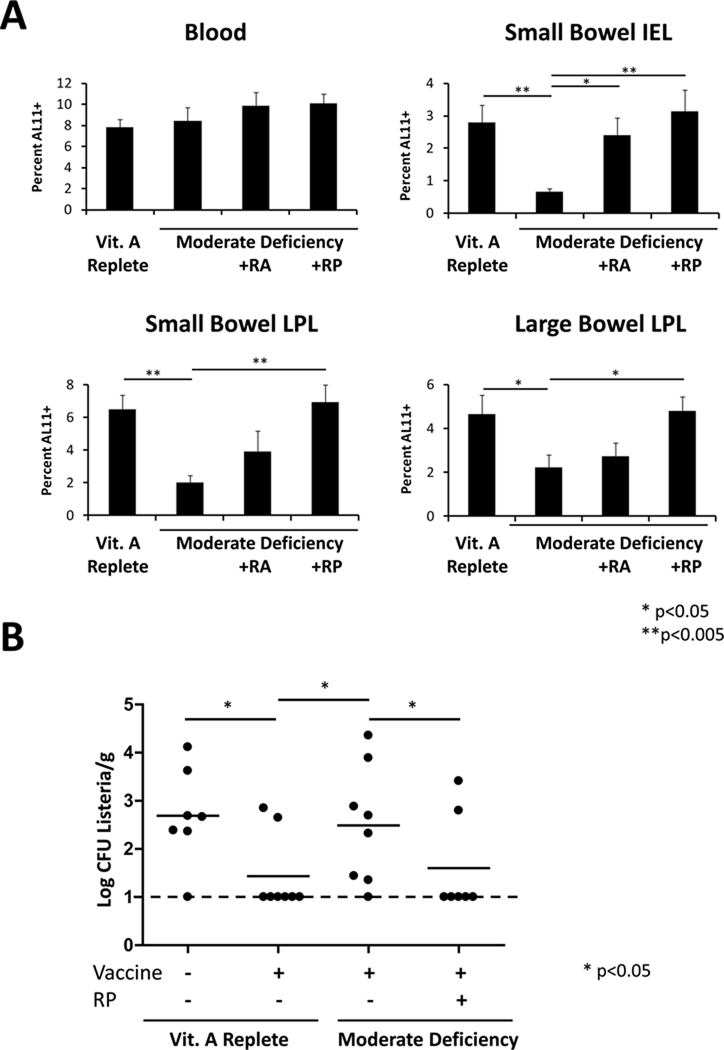
Vitamin A deficiency is highly prevalent in much of the developing world, where vaccination programs are of paramount importance to public health. However, the impact of vitamin A deficiency on the immunogenicity and protective efficacy of vaccines has not been defined previously. In this article, we show that the vitamin A metabolite retinoic acid is critical for trafficking of vaccine-elicited T lymphocytes to the gastrointestinal mucosa and for vaccine protective efficacy in mice. Moderate vitamin A deficiency abrogated Ag-specific T lymphocyte trafficking to the gastrointestinal tract, gastrointestinal cellular immune responses, and protection against a mucosal challenge following immunization with a recombinant adenovirus vaccine vector. Oral vitamin A supplementation as well as retinoic acid administration fully restored the mucosal immune responses and vaccine protective efficacy. These data suggest that oral vitamin A supplementation may be important for optimizing the success of vaccines against HIV-1 and other mucosal pathogens in the developing world, highlighting a critical relationship between host nutritional status and vaccine efficacy.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- WHO. Global prevalence of vitamin A deficiency in populations at risk 1995–2005: WHO global database on vitamin A deficiency. Geneva: World Health Organization; 2009.
-
- DeCicco KL, Zolfaghari R, Li N, Ross AC. Retinoic acid and polyriboinosinic acid act synergistically to enhance the antibody response to tetanus toxoid during vitamin A deficiency: possible involvement of interleukin-2 receptor-beta, signal transducer and activator of transcription-1, and interferon regulatory factor-1. J. Infect. Dis. 2000;182 Suppl 1:S29–S36. - PubMed
-
- Ross AC. Vitamin A deficiency and retinoid repletion regulate the antibody response to bacterial antigens and the maintenance of natural killer cells. Clin. Immunol. Immunopathol. 1996;80:S63–S72. - PubMed
-
- Rahman MM, Mahalanabis D, Hossain S, Wahed MA, Alvarez JO, Siber GR, Thompson C, Santosham M, Fuchs GJ. Simultaneous vitamin A administration at routine immunization contact enhances antibody response to diphtheria vaccine in infants younger than six months. J. Nutr. 1999;129:2192–2195. - PubMed
-
- Bhaskaram P, Rao KV. Enhancement in seroconversion to measles vaccine with simultaneous administration of vitamin A in 9-months-old Indian infants. Indian J. Pediatr. 1997;64:503–509. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
