

Functional definition and characterization of acute traumatic coagulopathy
- PMID: 21765358
- PMCID: PMC3223409
- DOI: 10.1097/CCM.0b013e3182281af5
Functional definition and characterization of acute traumatic coagulopathy
Abstract
Objective: To identify an appropriate diagnostic tool for the early diagnosis of acute traumatic coagulopathy and validate this modality through prediction of transfusion requirements in trauma hemorrhage.
Design: Prospective observational cohort study.
Setting: Level 1 trauma center.
Patients: Adult trauma patients who met the local criteria for full trauma team activation. Exclusion criteria included emergency department arrival >2 hrs after injury, >2000 mL of intravenous fluid before emergency department arrival, or transfer from another hospital.
Interventions: None.
Measurements: Blood was collected on arrival in the emergency department and analyzed with laboratory prothrombin time, point-of-care prothrombin time, and rotational thromboelastometry. Prothrombin time ratio was calculated and acute traumatic coagulopathy defined as laboratory prothrombin time ratio >1.2. Transfusion requirements were recorded for the first 12 hrs following admission.
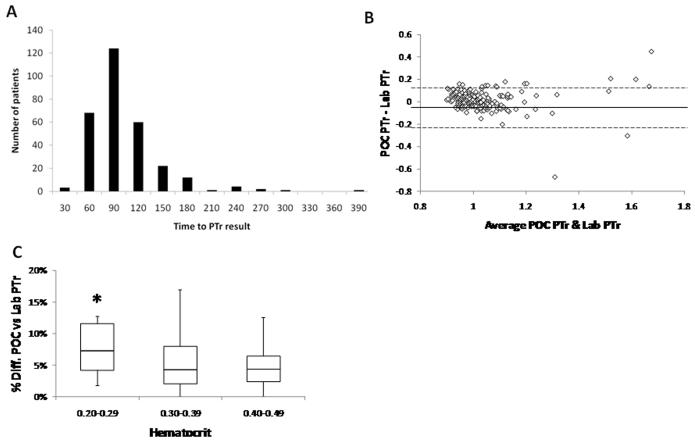
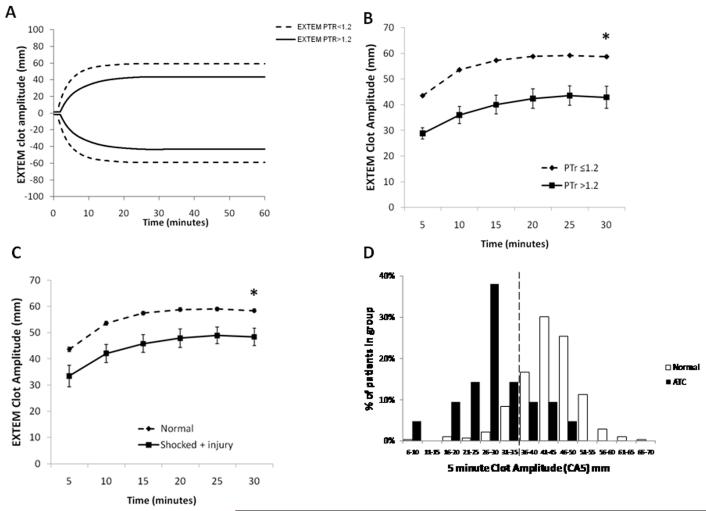
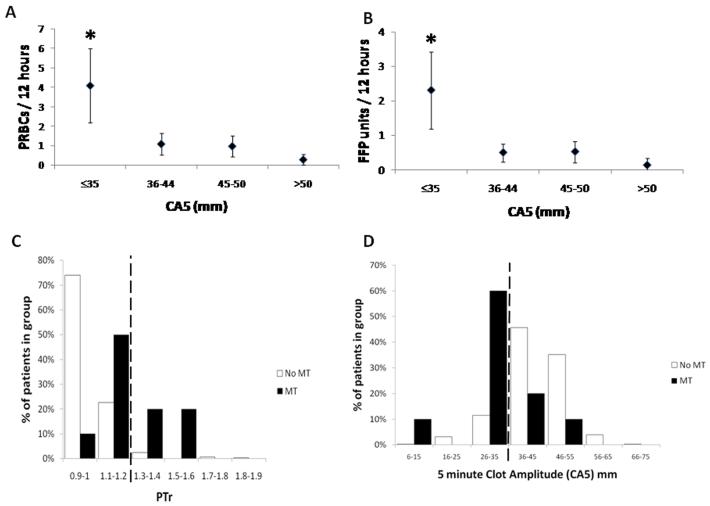
Main results: Three hundred patients were included in the study. Laboratory prothrombin time results were available at a median of 78 (62-103) mins. Point-of-care prothrombin time ratio had reduced agreement with laboratory prothrombin time ratio in patients with acute traumatic coagulopathy, with 29% false-negative results. In acute traumatic coagulopathy, the rotational thromboelastometry clot amplitude at 5 mins was diminished by 42%, and this persisted throughout clot maturation. Rotational thromboelastometry clotting time was not significantly prolonged. Clot amplitude at a 5-min threshold of ≤35 mm had a detection rate of 77% for acute traumatic coagulopathy with a false-positive rate of 13%. Patients with clot amplitude at 5 mins ≤35 mm were more likely to receive red cell (46% vs. 17%, p < .001) and plasma (37% vs. 11%, p < .001) transfusions. The clot amplitude at 5 mins could identify patients who would require massive transfusion (detection rate of 71%, vs. 43% for prothrombin time ratio >1.2, p < .001).
Conclusions: In trauma hemorrhage, prothrombin time ratio is not rapidly available from the laboratory and point-of-care devices can be inaccurate. Acute traumatic coagulopathy is functionally characterized by a reduction in clot strength. With a threshold of clot amplitude at 5 mins of ≤35 mm, rotational thromboelastometry can identify acute traumatic coagulopathy at 5 mins and predict the need for massive transfusion.
Figures
References
-
- Sauaia A, Moore FA, Moore EE, Moser KS, Brennan R, Read RA, et al. Epidemiology of trauma deaths: a reassessment. J Trauma. 1995 Feb;38(2):185–93. - PubMed
-
- Brohi K, Singh J, Heron M, Coats T. Acute traumatic coagulopathy. J Trauma. 2003 Jun;54(6):1127–30. - PubMed
-
- Maegele M, Lefering R, Yucel N, Tjardes T, Rixen D, Paffrath T, et al. Early coagulopathy in multiple injury: an analysis from the German Trauma Registry on 8724 patients. Injury. 2007 Mar;38(3):298–304. - PubMed
-
- MacLeod JB, Lynn M, McKenney MG, Cohn SM, Murtha M. Early coagulopathy predicts mortality in trauma. J Trauma. 2003 Jul;55(1):39–44. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
