

THE ROLE OF β-ADRENERGIC RECEPTORS IN HEART FAILURE: DIFFERENTIAL REGULATION OF CARDIOTOXICITY AND CARDIOPROTECTION
- PMID: 21765627
- PMCID: PMC3135901
- DOI: 10.1016/j.ppedcard.2010.11.007
THE ROLE OF β-ADRENERGIC RECEPTORS IN HEART FAILURE: DIFFERENTIAL REGULATION OF CARDIOTOXICITY AND CARDIOPROTECTION
Abstract
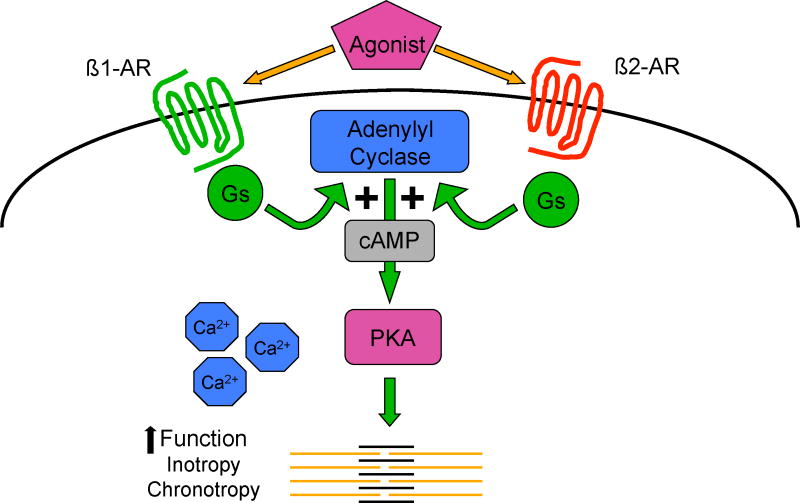
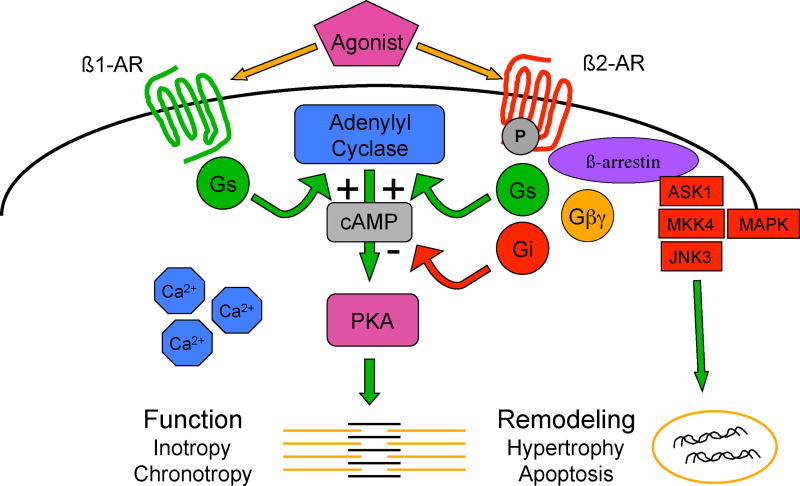
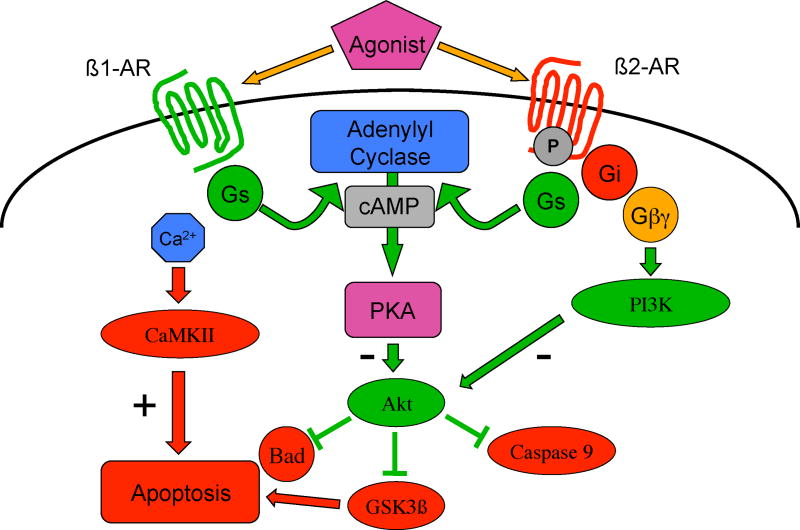
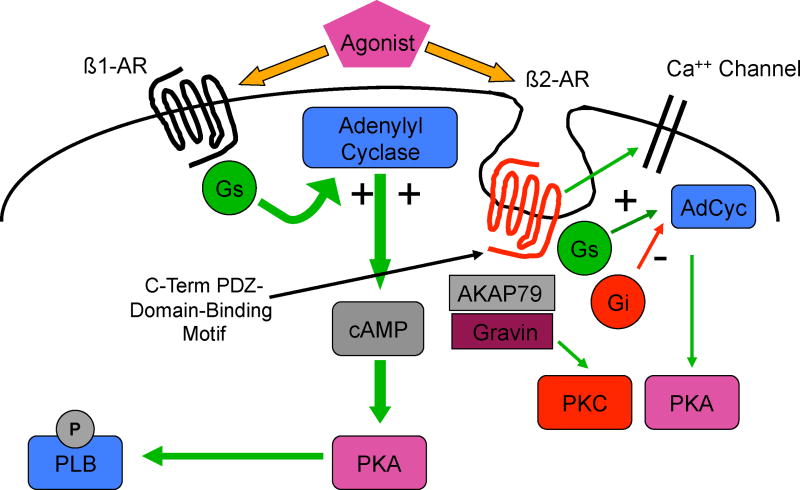
β-adrenergic receptor blockers have demonstrated significant survival benefit and have become standard therapy for adults with dilated cardiomyopathy, although their efficacy in pediatric patients is still unproven. Recent data suggests that the two major cardiac β-adrenergic receptor subtypes (β1 and β2) couple differentially to intracellular signaling pathways regulating contractility and remodeling. This has led some to suggest that the β1 receptor is the "cardiotoxic subtype" whereas the β2 receptor is "cardioprotective." Given this paradigm, there could be situations where subtype selective β-blockade or even subtype selective β-stimulation might be beneficial. However, since most of these studies have been performed in isolated cardiomyocytes, their application to clinical practice is unclear. To better understand the roles of β1- vs. β2-receptors in the pathogenesis of clinical cardiomyopathy, we and others have taken advantage of several well-characterized murine models of cardiovascular disease. These studies demonstrate that β-receptor regulation of the balance between cardioprotection and cardiotoxicity is even more complex than previously appreciated: the role of each β-receptor subtype may vary depending on the specific cardiac stressor involved (e.g. ischemia, pressure overload, genetic mutation, cardiotoxin). Furthermore, the remodeling effects of β-receptor signaling have a temporal component, depending on whether a cardiac stress is acute vs. chronic.
Figures
References
-
- Benedict C, Shelton B, Johnstone D, Francis G, Greenberg B, Konstam M, et al. Prognostic significance of plasma norepinephrine in patients with asymptomatic left ventricular dysfunction. SOLVD Investigators. Circulation. 1996;94:690–7. - PubMed
-
- Francis G, Cohn J, Johnson G, Rector T, Goldman S, Simon A. Plasma norepinephrine, plasma renin activity, and congestive heart failure: relations to survival and the effects of therapy in V-HeFT II. Circulation. 1993;87(Suppl VI):VI-40–8. - PubMed
-
- Hoffman BB, Lefkowitz RJ. Adrenergic receptors in the heart. Annu Rev Physiol. 1982;44:475–84. - PubMed
-
- Hausdorff WP, Caron MG, Lefkowitz RJ. Turning off the signal: desensitization of beta-adrenergic receptor function. FASEB J. 1990 Aug;4(11):2881–9. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials