

Observational study of the clinical efficacy of voriconazole and its relationship to plasma concentrations in patients
- PMID: 21768513
- PMCID: PMC3186950
- DOI: 10.1128/AAC.01083-10
Observational study of the clinical efficacy of voriconazole and its relationship to plasma concentrations in patients
Erratum in
- Antimicrob Agents Chemother. 2011 Nov;55(11):5415
Abstract
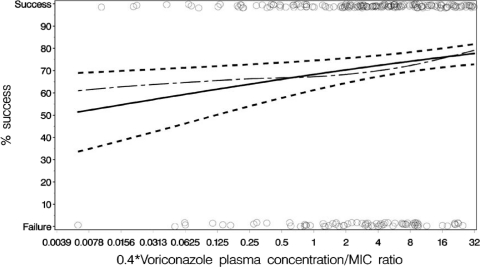
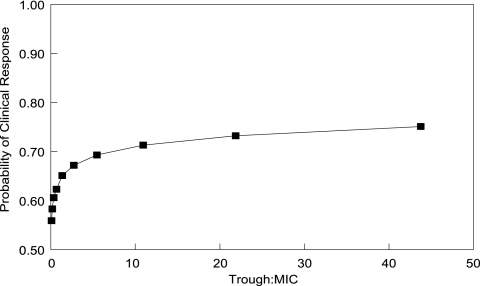
Voriconazole is approved for treating invasive fungal infections. We examined voriconazole exposure-response relationships for patients from nine published clinical trials. The relationship between the mean voriconazole plasma concentration (C(avg)) and clinical response and between the free C(avg)/MIC ratio versus the clinical response were explored using logistic regression. The impact of covariates on response was also assessed. Monte Carlo simulation was used to estimate the relationship between the trough concentration/MIC ratio and the probability of response. The covariates individually related to response were as follows: study (P < 0.001), therapy (primary/salvage, P < 0.001), primary diagnosis (P < 0.001), race (P = 0.004), baseline bilirubin (P < 0.001), baseline alkaline phosphatase (P = 0.014), and pathogen (yeast/mold, P < 0.001). The C(avg) for 72% of the patients was 0.5 to 5.0 μg/ml, with the maximum response rate (74%) at 3.0 to 4.0 μg/ml. The C(avg) showed a nonlinear relationship to response (P < 0.003), with a lower probability at the extremes. For patients with C(avg) < 0.5 μg/ml, the response rate was 57%. The lowest response rate (56%) was seen with a C(avg) ≥ 5.0 μg/ml (18% of patients) and was associated with significantly lower mold infection responses compared to yeasts (P < 0.001) but not with voriconazole toxicity. Higher free C(avg)/MIC ratios were associated with a progressively higher probability of response. Monte Carlo simulation suggested that a trough/MIC ratio of 2 to 5 is associated with a near-maximal probability of response. The probability of response is lower at the extremes of C(avg). Patients with higher free C(avg)/MIC ratios have a higher probability of clinical response. A trough/MIC ratio of 2 to 5 can be used as a target for therapeutic drug monitoring.
Figures

References
-
- Ally R., et al. 2001. A randomized, double-blind, double-dummy, multicenter trial of voriconazole and fluconazole in the treatment of esophageal candidiasis in immunocompromised patients. Clin. Infect. Dis. 33:1447–1454 - PubMed
-
- Andes D. 2004. Antifungal pharmacokinetics and pharmacodynamics: understanding the implications for antifungal drug resistance. Drug Resist. Updates 7:185–194 - PubMed
-
- Andes D. 2003. Pharmacokinetics and pharmacodynamics in the development of antifungal compounds. Curr. Opin. Invest. Drugs 4:991–998 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
