

Cortical calcification in Sturge-Weber Syndrome on MRI-SWI: relation to brain perfusion status and seizure severity
- PMID: 21769978
- PMCID: PMC3176926
- DOI: 10.1002/jmri.22687
Cortical calcification in Sturge-Weber Syndrome on MRI-SWI: relation to brain perfusion status and seizure severity
Abstract
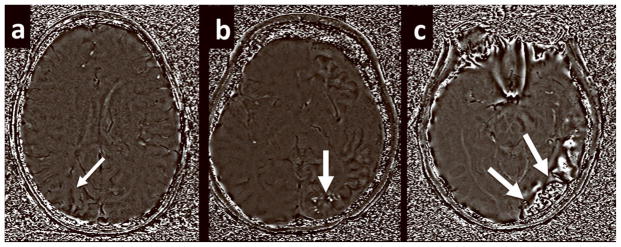
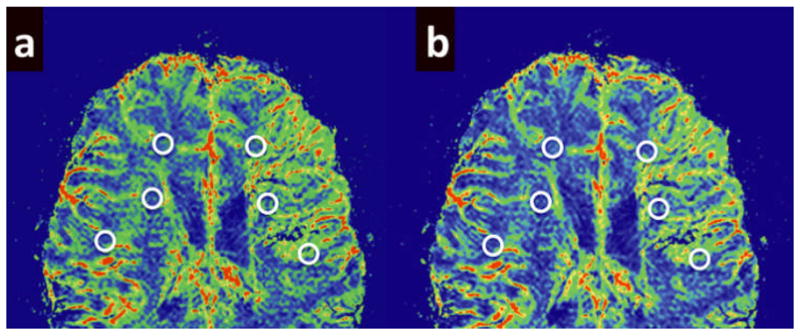
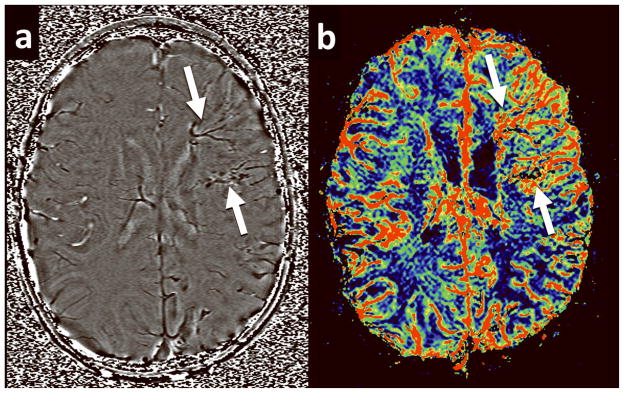
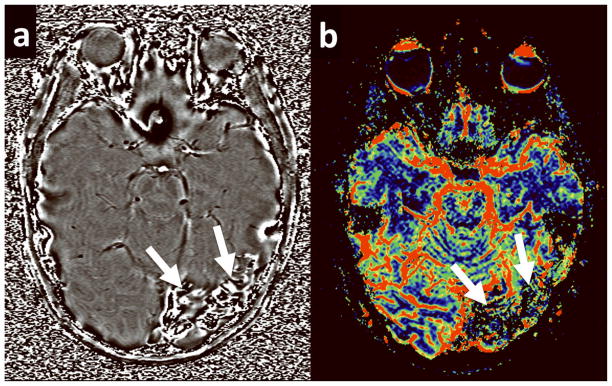
Purpose: To determine the relationship between calcified cortex and perfusion status of white matter and seizure severity in patients with Sturge-Weber Syndrome (SWS), a sporadic neurocutaneous disorder characterized by a leptomeningeal angioma, progressive brain ischemia, and a high incidence of seizures using susceptibility weighted imaging (SWI) and dynamic susceptibility contrast-enhanced perfusion weighted imaging (DSC-PWI).
Materials and methods: Fifteen children (ages: 0.9-10 years) with unilateral SWS prospectively underwent magnetic resonance imaging (MRI). The degree of cortical calcification was assessed using SWI while perfusion status was quantified using DSC-PWI images (asymmetries of various perfusion parameters). Comparisons between calcification, perfusion status, and seizure variables were performed.
Results: Patients with severely calcified cortex demonstrated significantly lower perfusion in the ipsilateral white matter (mean asymmetry: -0.52 ± 0.22) as compared to patients with only mildly calcified cortex or no calcification (mean asymmetry: 0.08 ± 0.25). Patients with severely calcified cortex also suffered from a higher seizure burden (a composite measure of seizure frequency and epilepsy duration; P = 0.01) and a trend for earlier seizure onset and longer epilepsy duration.
Conclusion: Severe calcification in the affected hemisphere is related to severely decreased perfusion in underlying white matter and is associated with more severe epilepsy in SWS patients.
Copyright © 2011 Wiley-Liss, Inc.
Figures
References
-
- Comi A. Topical Review: Pathophysiology of Sturge-Weber Syndrome. J Child Neurol. 2003;18:509–516. - PubMed
-
- Sujansky E, Conradi S. Outcome of Sturge-Weber syndrome in 53 adults. Am J Med Genet. 2005;57:35–45. - PubMed
-
- Sujansky E, Conradi S. Sturge-Weber Syndrome: Age of Onset of Seizures and Glaucoma and the Prognosis for Affected Children. J Child Neurol. 1995;10:49–58. - PubMed
-
- Roach ES, Riela AR, Chugani HT, Shinar S, Bodensteiner JB, Freeman J. Sturge-Weber Syndrome: Recommendations for Surgery. J Child Neurol. 1994;9:190–192. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
