

Oliguria as predictive biomarker of acute kidney injury in critically ill patients
- PMID: 21771324
- PMCID: PMC3387614
- DOI: 10.1186/cc10318
Oliguria as predictive biomarker of acute kidney injury in critically ill patients
Abstract
Introduction: During critical illness, oliguria is often used as a biomarker of acute kidney injury (AKI). However, its relationship with the subsequent development of AKI has not been prospectively evaluated.
Methods: We documented urine output and daily serum creatinine concentration in patients admitted for more than 24 hours in seven intensive care units (ICUs) from six countries over a period of two to four weeks. Oliguria was defined by a urine output < 0.5 ml/kg/hr. Data were collected until the occurrence of creatinine-defined AKI (AKI-Cr), designated by RIFLE-Injury class or greater using creatinine criteria (RIFLE-I[Cr]), or until ICU discharge. Episodes of oliguria were classified by longest duration of consecutive oliguria during each day were correlated with new AKI-Cr the next day, examining cut-offs for oliguria of greater than 1,2,3,4,5,6, or 12 hr duration,
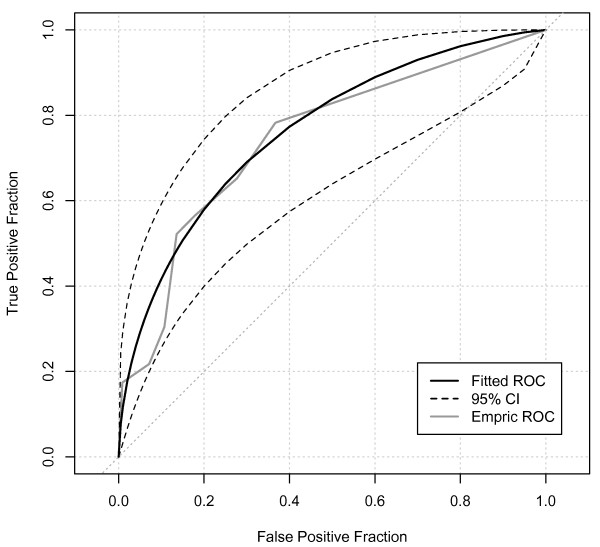
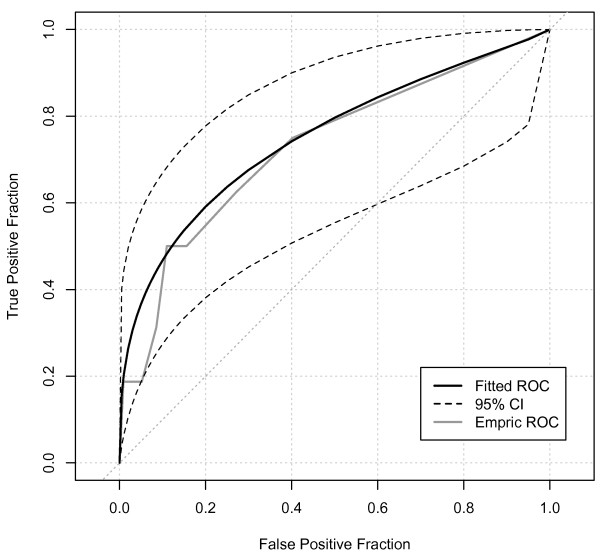
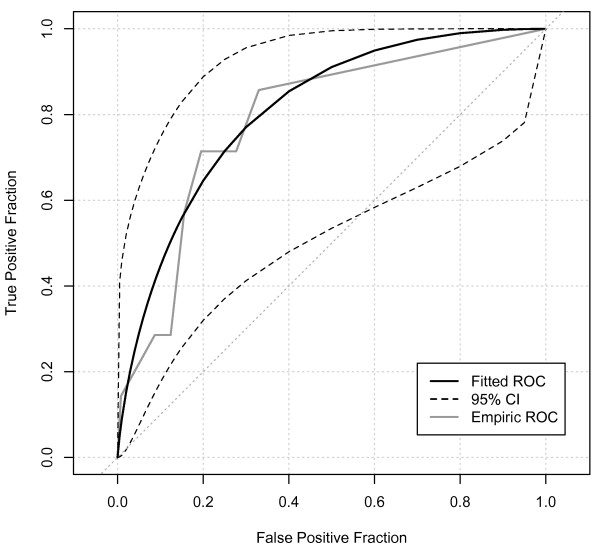
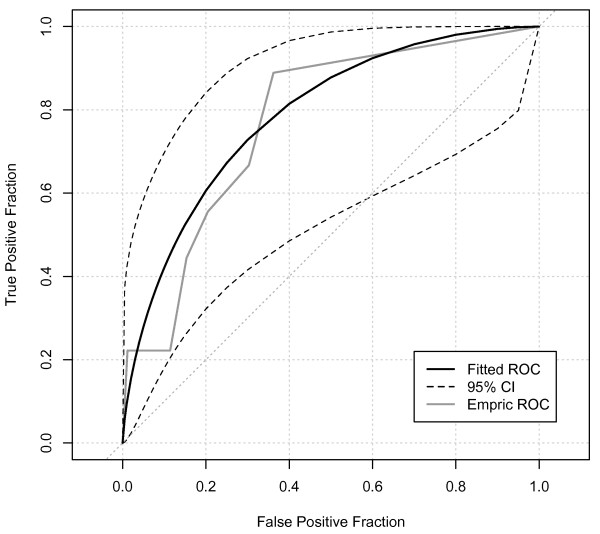
Results: We studied 239 patients during 723 days. Overall, 32 patients had AKI on ICU admission, while in 23, AKI-Cr developed in ICU. Oliguria of greater than one hour was significantly associated with AKI-Cr the next day. On receiver-operator characteristic area under the curve (ROCAUC) analysis, oliguria showed fair predictive ability for AKI-Cr (ROCAUC = 0.75; CI:0.64-0.85). The presence of 4 hrs or more oliguria provided the best discrimination (sensitivity 52% (0.31-0.73%), specificity 86% (0.84-0.89%), positive likelihood ratio 3.8 (2.2-5.6), P < 0.0001) with negative predictive value of 98% (0.97-0.99). Oliguria preceding AKI-Cr was more likely to be associated with lower blood pressure, higher heart rate and use of vasopressors or inotropes and was more likely to prompt clinical intervention. However, only 30 of 487 individual episodes of oliguria preceded the new occurrence of AKI-Cr the next day.
Conclusions: Oliguria was significantly associated with the occurrence of new AKI-Cr, however oliguria occurred frequently compared to the small number of patients (~10%) developing AKI-Cr in the ICU, so that most episodes of oliguria were not followed by renal injury. Consequently, the occurrence of short periods (1-6 hr) of oliguria lacked utility in discriminating patients with incipient AKI-Cr (positive likelihood ratios of 2-4, with > 10 considered indicative of a useful screening test). However, oliguria accompanied by hemodynamic compromise or increasing vasopressor dose may represent a clinically useful trigger for other early biomarkers of renal injury.
Figures
References
-
- Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P. Acute Dialysis Quality Initiative workgroup. Acute renal failure - definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care. 2004;8:R204–212. doi: 10.1186/cc2872. - DOI - PMC - PubMed
-
- Rimmelé T, Kellum JA. Oliguria and fluid overload. Contrib Nephrol. 2010;164:39–45. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
