

The infarct core is well represented by the acute diffusion lesion: sustained reversal is infrequent
- PMID: 21772309
- PMCID: PMC3323290
- DOI: 10.1038/jcbfm.2011.102
The infarct core is well represented by the acute diffusion lesion: sustained reversal is infrequent
Abstract
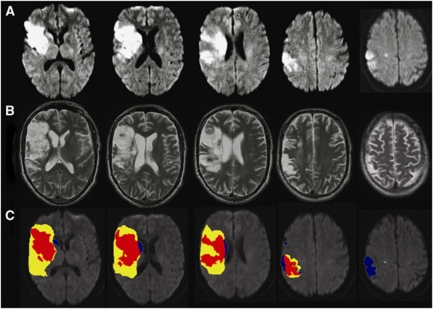
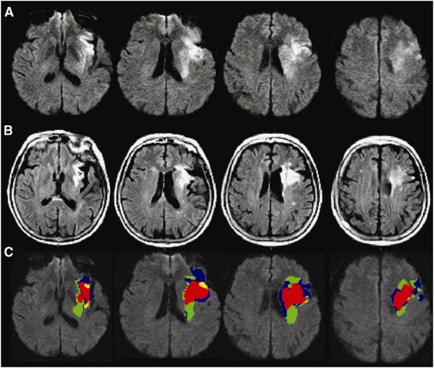
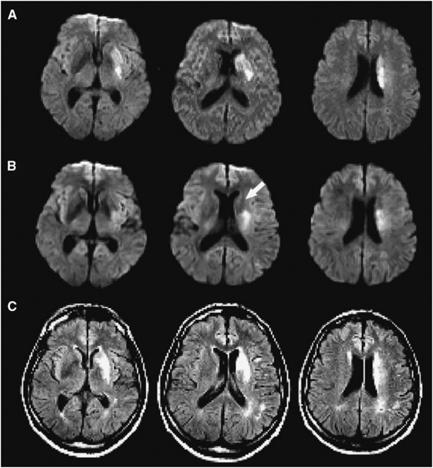
Diffusion-weighted imaging (DWI) is commonly used to assess irreversibly infarcted tissue but its accuracy is challenged by reports of diffusion lesion reversal (DLR). We investigated the frequency and implications for mismatch classification of DLR using imaging from the EPITHET (Echoplanar Imaging Thrombolytic Evaluation Trial) and DEFUSE (Diffusion and Perfusion Imaging Evaluation for Understanding Stroke Evolution) studies. In 119 patients (83 treated with IV tissue plasminogen activator), follow-up images were coregistered to acute diffusion images and the lesions manually outlined to their maximal visual extent in diffusion space. Diffusion lesion reversal was defined as voxels of acute diffusion lesion that corresponded to normal brain at follow-up (i.e., final infarct, leukoaraiosis, and cerebrospinal fluid (CSF) voxels were excluded from consideration). The appearance of DLR was visually checked for artifacts, the volume calculated, and the impact of adjusting baseline diffusion lesion volume for DLR volume on perfusion-diffusion mismatch analyzed. Median DLR volume reduced from 4.4 to 1.5 mL after excluding CSF/leukoaraiosis. Visual inspection verified 8/119 (6.7%) with true DLR, median volume 2.33 mL. Subtracting DLR from acute diffusion volume altered perfusion-diffusion mismatch (T(max)>6 seconds, ratio>1.2) in 3/119 (2.5%) patients. Diffusion lesion reversal between baseline and 3 to 6 hours DWI was also uncommon (7/65, 11%) and often transient. Clinically relevant DLR is uncommon and rarely alters perfusion-diffusion mismatch. The acute diffusion lesion is generally a reliable signature of the infarct core.
Figures
References
-
- Albers GW, Thijs VN, Wechsler L, Kemp S, Schlaug G, Skalabrin E, Bammer R, Kakuda W, Lansberg MG, Shuaib A, Coplin W, Hamilton S, Moseley M, Marks MP. Magnetic resonance imaging profiles predict clinical response to early reperfusion: the diffusion and perfusion imaging evaluation for understanding stroke evolution (DEFUSE) study. Ann Neurol. 2006;60:508–517. - PubMed
-
- Butcher K, Parsons M, Allport L, Lee SB, Barber PA, Tress B, Donnan GA, Davis SM. Rapid assessment of perfusion-diffusion mismatch. Stroke. 2008;39:75–81. - PubMed
-
- Chalela JA, Kang DW, Luby M, Ezzeddine M, Latour LL, Todd JW, Dunn B, Warach S. Early magnetic resonance imaging findings in patients receiving tissue plasminogen activator predict outcome: insights into the pathophysiology of acute stroke in the thrombolysis era. Ann Neurol. 2004;55:105–112. - PubMed
-
- Chemmanam T, Campbell BCV, Christensen S, Nagakane Y, Desmond PM, Bladin CF, Parsons MW, Levi CR, Barber PA, Donnan GA, Davis SM. Ischemic diffusion lesion reversal is uncommon and rarely alters perfusion-diffusion mismatch. Neurology. 2010;75:1040–1047. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
