

Folliculitis et perifolliculitis capitis abscedens et suffodiens controlled with a combination therapy: systemic antibiosis (metronidazole plus clindamycin), dermatosurgical approach, and high-dose isotretinoin
- PMID: 21772598
- PMCID: PMC3132914
- DOI: 10.4103/0019-5154.82492
Folliculitis et perifolliculitis capitis abscedens et suffodiens controlled with a combination therapy: systemic antibiosis (metronidazole plus clindamycin), dermatosurgical approach, and high-dose isotretinoin
Abstract
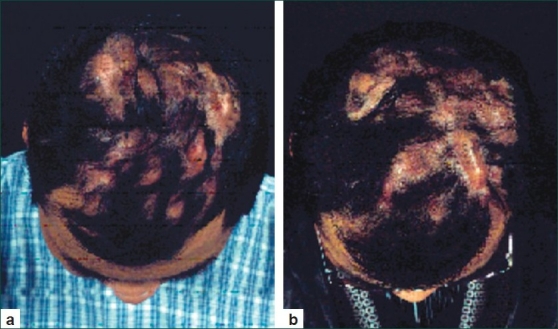
Folliculitis et perifolliculitis capitis abscedens et suffodiens is a rare disease of unknown etiology. It is a suppurative process that involves the scalp, eventually resulting in extensive scarring and irreversible alopecia. The condition is also known as 'acne necrotica miliaris' or 'Proprionibacterium' folliculitis. Most often the disease affects men of African-American or African-Caribbean descent between 20 and 40 years of age. The clinical picture is determined by fluctuating painful fistule-forming conglomerates of abscesses in the region of the occipital scalp. The cause of scalp folliculitis is not well understood. It is generally considered to be an inflammatory reaction to components of the hair follicle, particularly the micro-organisms. These include: bacteria (especially Propionibacterium acnes, but in severe cases, also Staphylococcus aureus), Yeasts (Malassezia species) and mites (Demodex folliculorum). The initial histopathologic finding is an exclusively neutrophilic infiltration followed by a granulomatous infiltrate. The treatment of the disease is usually difficult and often disappointing. Successful treatment with isotretinoin 1 mg/kg body mass could be achieved only after regular systematic administration in the course of 3-4 months. Here we describe a patient with eruptive purulent form of the disease, which has been controlled with combination therapy: systemic antibiosis with metronidazole and clindamycin, dermatosurgical removal of single nodular formations, and isotretinoin 1 mg/kg body mass for 3-5 months.
Keywords: Acne conglobata; Candida; Hoffmann; Spritzer; isotretinoin.
Conflict of interest statement
Figures

References
-
- Spritzer L. Dermatitis follicularis et perifollicularis conglobata. Dermatol Zeitschrift. 1903;10:109–20.
-
- Hoffmann E. Folliculitis et perifolliculitis capitis abscedens et suffodiens: case presentation. Dermatol Zeitschrift. 1908;15:122–3.
-
- Luderschmidt C, Klövekorn W. Systemic inflammatory reactions and extracutaneous manifestations of Acne vulgaris. Z Hautkr. 1986;61:617–21. - PubMed
-
- Curry SS, Gaither DH, King LE., Jr Squamous cell carcinoma arising in dissecting perifolliculitis of the scalp.A case report and review of secondary squamous cell carcinomas. J Am Acad Dermatol. 1981;4:673–8. - PubMed
-
- Gilliam AC, Lessin SR, Wilson DM, Salhany KE. Folliculotropic mycosis fungoides with large-cell transformation presenting as dissecting cellulitis of the scalp. J Cutan Pathol. 1997;24:169–75. - PubMed
LinkOut - more resources
Full Text Sources