Predictors of post-caesarean section pain and analgesic consumption
- PMID: 21772677
- PMCID: PMC3127296
- DOI: 10.4103/0970-9185.81822
Predictors of post-caesarean section pain and analgesic consumption
Abstract
Background: Ideally, the intensity of postoperative pain should be predicted so as to customize analgesia. The objective of this study was to investigate whether preoperative electrical and pressure pain assessment can predict post-caesarean section pain and analgesic requirement.
Materials and methods: A total of 65 subjects scheduled for elective caesarean section, who gave written informed consent, were studied. Preoperatively, PainMatcher(®) was used to evaluate electrical pain threshold, while manual PainTest™ FPN 100 Algometer and digital PainTest™ FPX 25 Algometer determined pressure pain threshold and tolerance. Postoperatively, numerical rating scales were used to assess pain at regular time intervals. Patients received intramuscular pethidine (100mg, 6 hourly), rectal diclofenac (100mg, 12 hourly), and oral paracetamol (1g, p.r.n.) for pain relief. Statistical analysis was conducted using PASW Statistics 18 software.
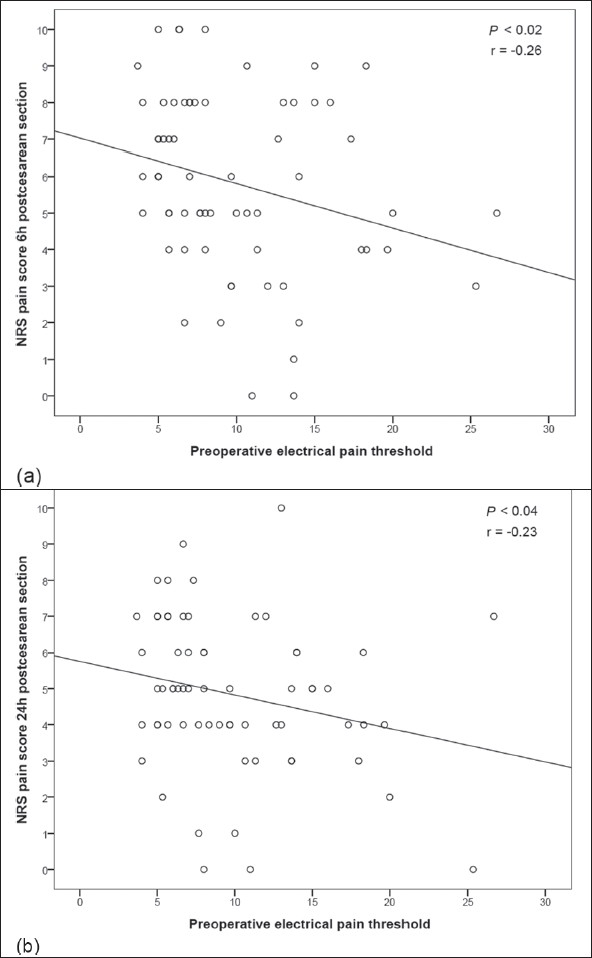
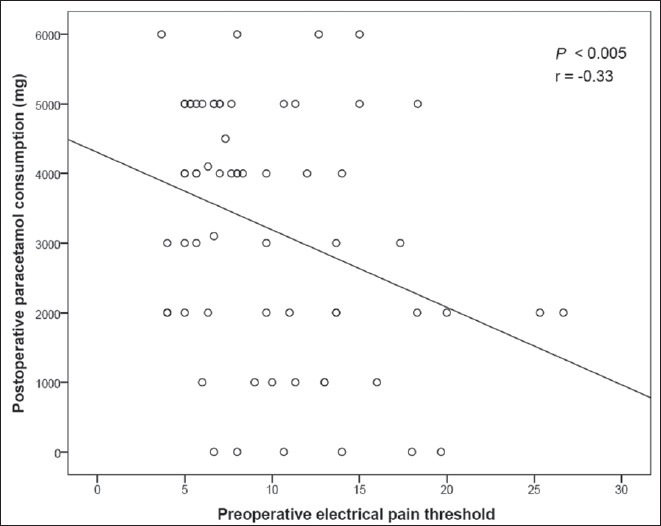
Results: Preoperative electrical pain threshold correlated significantly with post-caesarean pain scores at 6 and 24 hours (r = -0.26, P < 0.02; r = -0.23, P < 0.04, respectively), and with the quantity of paracetamol consumed by the patient within 48 hours of surgery (r = -0.33, P < 0.005). Preoperative pressure pain tolerance measured by PainTest™ FPX 25 Algometer was significantly correlated with pain scores 6 hours postsurgery (r = -0.21, P < 0.05). Pain scores 6 hours post-caesarean section correlated significantly with anesthesia-general or spinal (F = 4.22, v(1) = 1, v(2) = 63, P < 0.05).
Conclusions: The predictive methods proposed may aid in identifying patients at greater risk for postoperative pain. Electrical pain threshold could be useful in personalizing the postoperative analgesic protocol.
Keywords: Analgesia; caesarean section; general anesthesia; pain threshold; postoperative pain; spinal anesthesia.
Conflict of interest statement
Figures

References
-
- Granot M, Lowenstein L, Yarnitsky D, Tamir A, Zimmer E. Post-caesarean section pain prediction by preoperative experimental pain assessment. Anesthesiology. 2003;98:1422–6. - PubMed
-
- Hsu Y, Somma J, Hung Y, Tsai P, Yang C, Chen C. Predicting postoperative pain by preoperative pressure pain assessment. Anesthesiology. 2005;103:613–8. - PubMed
-
- Pan PH, Coghill R, Houle TT, Seid MH, Lindel WM, Parker RL, et al. Multifactorial preoperative predictors for post-caesarean section pain and analgesic requirement. Anesthesiology. 2006;104:417–25. - PubMed
-
- Stener-Victorin E, Kowalski J, Lundeberg T. A new highly reliable instrument for the assessment of pre- and postoperative gynaecological pain. Anesth Analg. 2002;95:151–7. - PubMed