

Optimal monitoring time interval between DXA measures in children
- PMID: 21773995
- PMCID: PMC3200454
- DOI: 10.1002/jbmr.473
Optimal monitoring time interval between DXA measures in children
Abstract
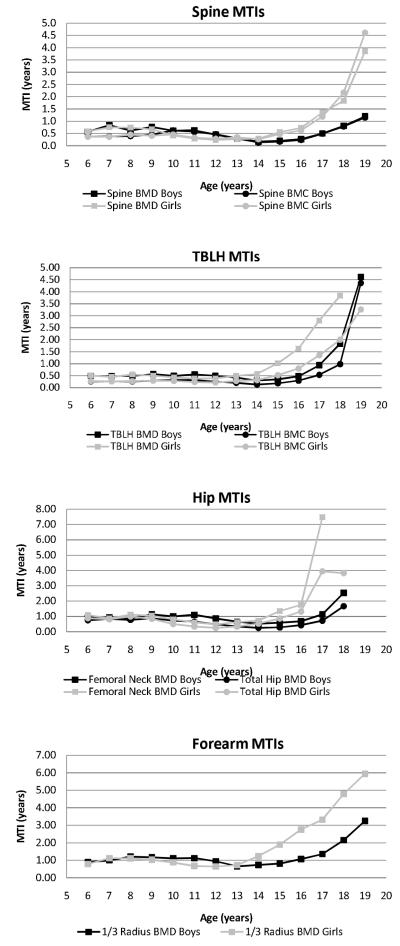
The monitoring time interval (MTI) is the expected time in years necessary to identify a change between two measures that exceeds the measurement error. Our purpose was to determine MTI values for dual-energy X-ray absorptiometry (DXA) scans in normal healthy children, according to age, sex, and skeletal site. 2014 children were enrolled in the Bone Mineral Density in Childhood Study and had DXA scans of the lumbar spine, total hip, nondominant forearm, and whole body. Measurements were obtained annually for seven visits from 2002 to 2010. Annualized rates of change were calculated by age and sex for all bone regions. A subgroup of 155 children ages 6 to 16 years (85 boys) had duplicate scans for calculation of scan precision. The bone mineral density (BMD) regions of interest included the spine, total body less head (TBLH), total hip, femoral neck, and one-third radius. Bone mineral content (BMC) was also evaluated for the spine and TBLH. The percent coefficient of variation (%CV) and MTI were calculated for each measure as a function of age and sex. The MTI values were substantially less than 1 year for the TBLH and spine BMD and BMC for boys ≤ 17 years and girls ≤ 15 years. The hip and one-third radius MTIs were generally 1 year in the same group. MTI values as low as 3 months were found during the peak growth years. However, the MTI values in late adolescence for all regions were substantially longer and became nonsensical as each region neared the age for peak bone density. All four DXA measurement sites had reasonable (< 1 year) MTI values for boys ≤ 17 years and girls ≤ 15 years. MTI was neither useful nor stable in late adolescence and young adulthood. Alternative criteria to determine scan intervals must be used in this age range.
Copyright © 2011 American Society for Bone and Mineral Research.
Figures
References
-
- Gilsanz V. Bone density in children: a review of the available techniques and indications. Eur J Radiol. 1998;26(2):177–82. - PubMed
-
- Ellis KJ, Shypailo RJ, Pratt JA, Pond WG. Accuracy of dual-energy x-ray absorptiometry for body-composition measurements in children [see comments] Am J Clin Nutr. 1994;60(5):660–5. - PubMed
-
- Kolta S, Ravaud P, Fechtenbaum J, Dougados M, Roux C. Accuracy and precision of 62 bone densitometers using a European Spine Phantom. Osteoporos Int. 1999;10(1):14–9. - PubMed
-
- Kalkwarf HJ, Zemel BS, Gilsanz V, Lappe JM, Horlick M, Oberfield S, Mahboubi S, Fan B, Frederick MM, Winer K, Shepherd JA. The bone mineral density in childhood study: bone mineral content and density according to age, sex, and race. J Clin Endocrinol Metab. 2007;92(6):2087–99. - PubMed
-
- Zemel B, Kalkwarf HJ, Gilsanz V, Lappe JM, Oberfield S, Shepherd JA, Frederick MM, Huang X, M. L, Mahboubi S, Hangartner T, Winer K. Revised Reference Curves for Bone Mineral Content and Density According to Age and Sex for Black and Non-Black Children: Results of The Bone Mineral Density in Childhood Study. Journal of Clinical Endocrinology & Metabolism. 2011 In Press. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
