

Carotid-wall intima-media thickness and cardiovascular events
- PMID: 21774709
- PMCID: PMC3153949
- DOI: 10.1056/NEJMoa1012592
Carotid-wall intima-media thickness and cardiovascular events
Abstract
Background: Intima-media thickness of the walls of the common carotid artery and internal carotid artery may add to the Framingham risk score for predicting cardiovascular events.
Methods: We measured the mean intima-media thickness of the common carotid artery and the maximum intima-media thickness of the internal carotid artery in 2965 members of the Framingham Offspring Study cohort. Cardiovascular-disease outcomes were evaluated for an average follow-up of 7.2 years. Multivariable Cox proportional-hazards models were generated for intima-media thickness and risk factors. We evaluated the reclassification of cardiovascular disease on the basis of the 8-year Framingham risk score category (low, intermediate, or high) after adding intima-media thickness values.
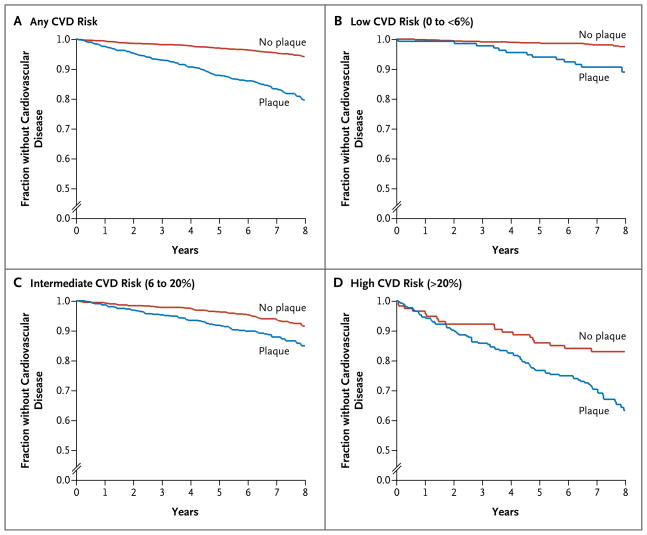
Results: A total of 296 participants had a cardiovascular event. The risk factors of the Framingham risk score predicted these events, with a C statistic of 0.748 (95% confidence interval [CI], 0.719 to 0.776). The adjusted hazard ratio for cardiovascular disease with a 1-SD increase in the mean intima-media thickness of the common carotid artery was 1.13 (95% CI, 1.02 to 1.24), with a nonsignificant change in the C statistic of 0.003 (95% CI, 0.000 to 0.007); the corresponding hazard ratio for the maximum intima-media thickness of the internal carotid artery was 1.21 (95% CI, 1.13 to 1.29), with a modest increase in the C statistic of 0.009 (95% CI, 0.003 to 0.016). The net reclassification index increased significantly after addition of intima-media thickness of the internal carotid artery (7.6%, P<0.001) but not intima-media thickness of the common carotid artery (0.0%, P=0.99). With the presence of plaque, defined as intima-media thickness of the internal carotid artery of more than 1.5 mm, the net reclassification index was 7.3% (P=0.01), with an increase in the C statistic of 0.014 (95% CI, 0.003 to 0.025).
Conclusions: The maximum internal and mean common carotid-artery intima-media thicknesses both predict cardiovascular outcomes, but only the maximum intima-media thickness of (and presence of plaque in) the internal carotid artery significantly (albeit modestly) improves the classification of risk of cardiovascular disease in the Framingham Offspring Study cohort. (Funded by the National Heart, Lung, and Blood Institute.).
Conflict of interest statement
Dr. Pencina reports receiving fees for board membership from Abbott. No other potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Cerebrovascular disorders: carotid-wall intima-media thickness, stroke recurrence, and β-blocker selectivity.J Neurol. 2011 Oct;258(10):1904-6. doi: 10.1007/s00415-011-6245-0. J Neurol. 2011. PMID: 21932126 No abstract available.
-
Carotid intima-media thickness and cardiovascular events.N Engl J Med. 2011 Oct 27;365(17):1640; author reply 1641-2. doi: 10.1056/NEJMc1109714. N Engl J Med. 2011. PMID: 22029988 No abstract available.
-
Carotid intima-media thickness and cardiovascular events.N Engl J Med. 2011 Oct 27;365(17):1640-1; author reply 1641-2. doi: 10.1056/NEJMc1109714. N Engl J Med. 2011. PMID: 22029989 No abstract available.
-
Carotid intima-media thickness and cardiovascular events.N Engl J Med. 2011 Oct 27;365(17):1641; author reply 1641-2. doi: 10.1056/NEJMc1109714. N Engl J Med. 2011. PMID: 22029990 No abstract available.
References
-
- Hodis HN, Mack WJ, LaBree L, et al. Reduction in carotid arterial wall thickness using lovastatin and dietary therapy: a randomized controlled clinical trial. Ann Intern Med. 1996;124:548–56. - PubMed
-
- O’Leary DH, Polak JF, Kronmal RA, et al. Thickening of the carotid wall: a marker for atherosclerosis in the elderly? Stroke. 1996;27:224–31. - PubMed
-
- O’Leary DH, Polak JF, Kronmal RA, Manolio TA, Burke GL, Wolfson SK., Jr Carotid-artery intima and media thickness as a risk factor for myocardial infarction and stroke in older adults. N Engl J Med. 1999;340:14–22. - PubMed
-
- Chambless LE, Heiss G, Folsom AR, et al. Association of coronary heart disease incidence with carotid arterial wall thickness and major risk factors: the Atherosclerosis Risk in Communities (ARIC) Study, 1987–1993. Am J Epidemiol. 1997;146:483–94. - PubMed
-
- Bots ML, Hoes AW, Koudstaal PJ, Hofman A, Grobbee DE. Common carotid intima-media thickness and risk of stroke and myocardial infarction: the Rotterdam Study. Circulation. 1997;96:1432–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical