

Constrictive bronchiolitis in soldiers returning from Iraq and Afghanistan
- PMID: 21774710
- PMCID: PMC3296566
- DOI: 10.1056/NEJMoa1101388
Constrictive bronchiolitis in soldiers returning from Iraq and Afghanistan
Erratum in
- N Engl J Med. 2011 Nov 3;365(18):1749
Abstract
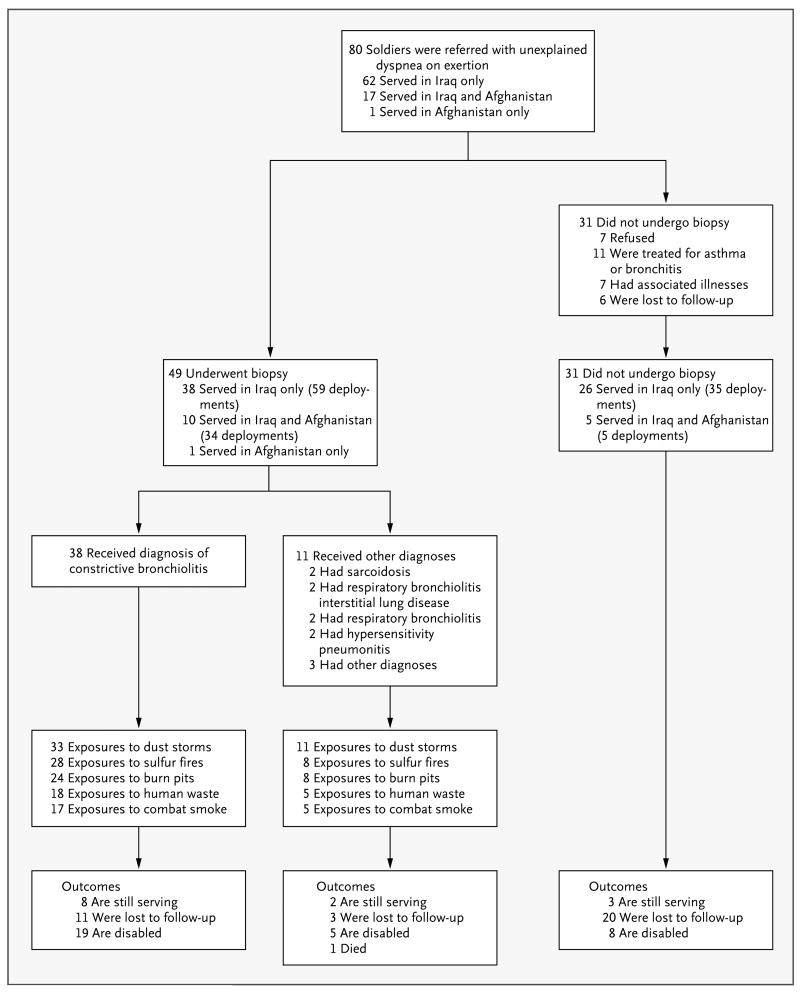
Background: In this descriptive case series, 80 soldiers from Fort Campbell, Kentucky, with inhalational exposures during service in Iraq and Afghanistan were evaluated for dyspnea on exertion that prevented them from meeting the U.S. Army's standards for physical fitness.
Methods: The soldiers underwent extensive evaluation of their medical and exposure history, physical examination, pulmonary-function testing, and high-resolution computed tomography (CT). A total of 49 soldiers underwent thoracoscopic lung biopsy after noninvasive evaluation did not provide an explanation for their symptoms. Data on cardiopulmonary-exercise and pulmonary-function testing were compared with data obtained from historical military control subjects.
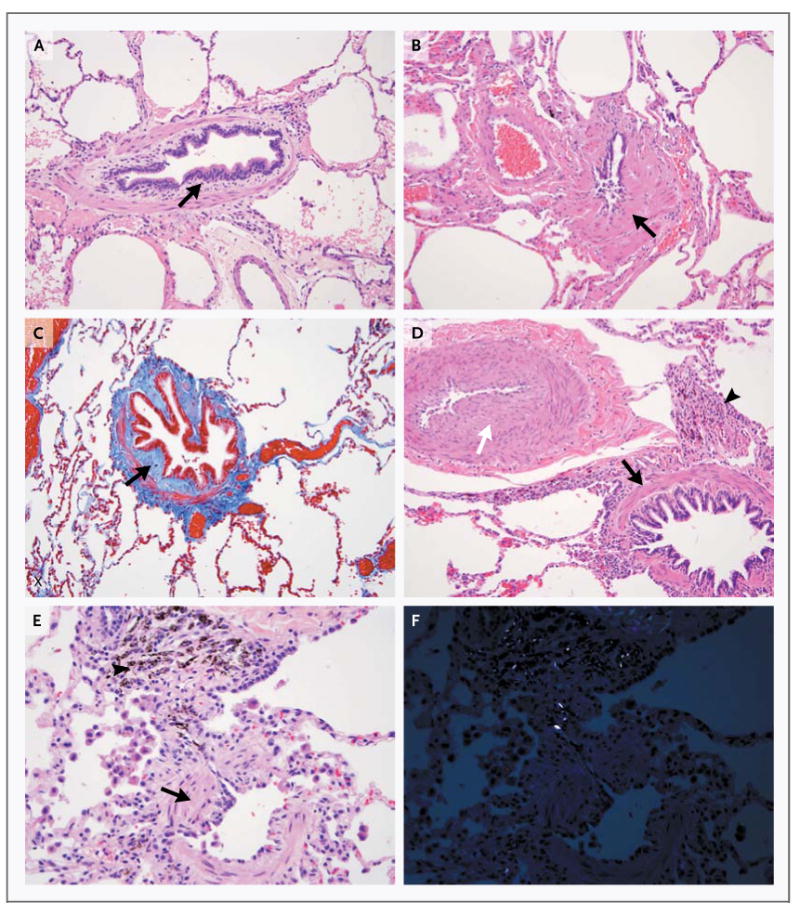
Results: Among the soldiers who were referred for evaluation, a history of inhalational exposure to a 2003 sulfur-mine fire in Iraq was common but not universal. Of the 49 soldiers who underwent lung biopsy, all biopsy samples were abnormal, with 38 soldiers having changes that were diagnostic of constrictive bronchiolitis. In the remaining 11 soldiers, diagnoses other than constrictive bronchiolitis that could explain the presenting dyspnea were established. All soldiers with constrictive bronchiolitis had normal results on chest radiography, but about one quarter were found to have mosaic air trapping or centrilobular nodules on chest CT. The results of pulmonary-function and cardiopulmonary-exercise testing were generally within normal population limits but were inferior to those of the military control subjects.
Conclusions: In 49 previously healthy soldiers with unexplained exertional dyspnea and diminished exercise tolerance after deployment, an analysis of biopsy samples showed diffuse constrictive bronchiolitis, which was possibly associated with inhalational exposure, in 38 soldiers.
Figures
Comment in
-
Constrictive bronchiolitis in soldiers.N Engl J Med. 2011 Nov 3;365(18):1743; author reply 1744-5. doi: 10.1056/NEJMc1109866. N Engl J Med. 2011. PMID: 22047574 No abstract available.
-
Constrictive bronchiolitis in soldiers.N Engl J Med. 2011 Nov 3;365(18):1743-4; author reply 1744-5. doi: 10.1056/NEJMc1109866. N Engl J Med. 2011. PMID: 22047575 No abstract available.
-
Constrictive bronchiolitis in soldiers.N Engl J Med. 2011 Nov 3;365(18):1744; author reply 1744-5. doi: 10.1056/NEJMc1109866. N Engl J Med. 2011. PMID: 22047576 No abstract available.
References
-
- Medinger AE, Chan TW, Arabian A, Rohatgi PK. Interpretive algorithms for the symptom-limited exercise test: assessing dyspnea in Persian Gulf veterans. Chest. 1998;113:612–8. - PubMed
-
- Smith B, Wong CA, Smith TC, Boyko EJ, Gackstetter GD, Ryan MAK. Newly reported respiratory symptoms and conditions among military personnel deployed to Iraq and Afghanistan: a prospective population-based study. Am J Epidemiol. 2009;170:1433–44. - PubMed
-
- The Iowa Persian Gulf Study Group. Self-reported illness and health status among Gulf War veterans: a population-based study. JAMA. 1997;277:238–45. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical