

Discontinuities in the human bone-PDL-cementum complex
- PMID: 21774982
- PMCID: PMC3185383
- DOI: 10.1016/j.biomaterials.2011.06.021
Discontinuities in the human bone-PDL-cementum complex
Abstract
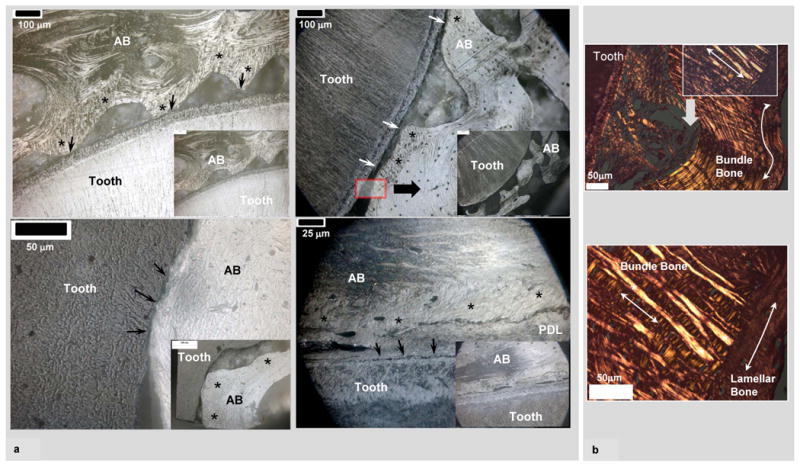
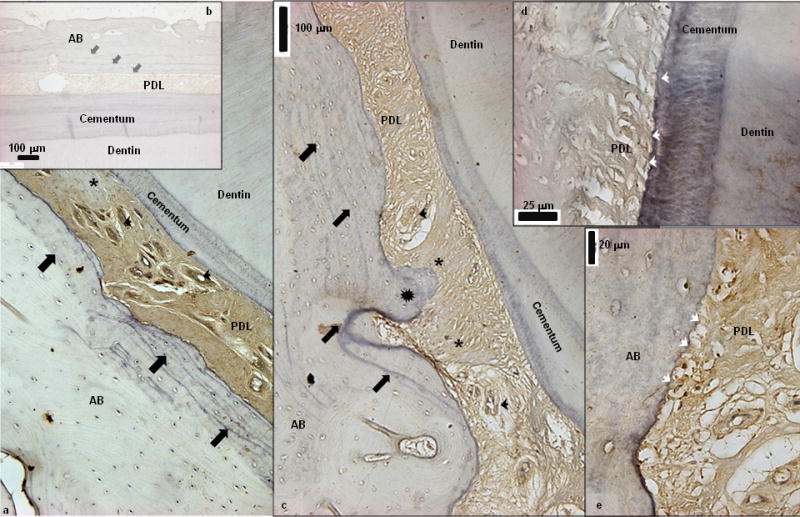
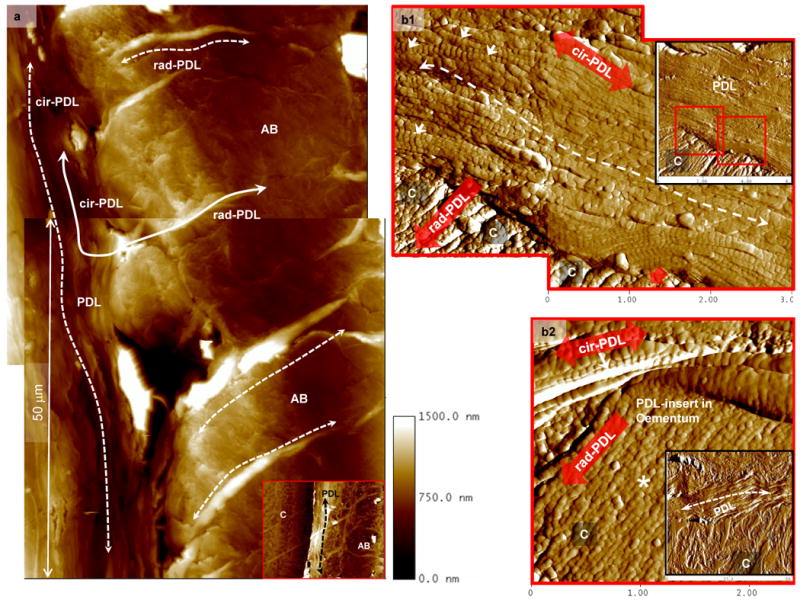
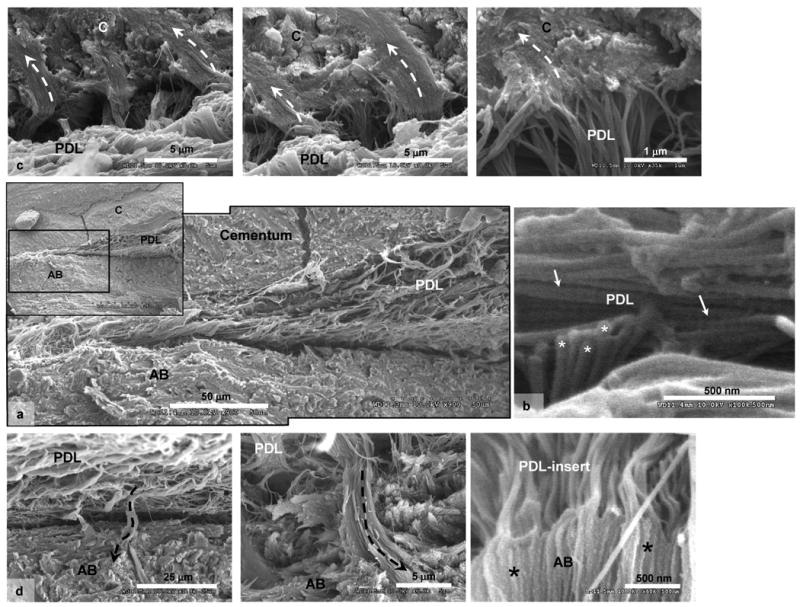
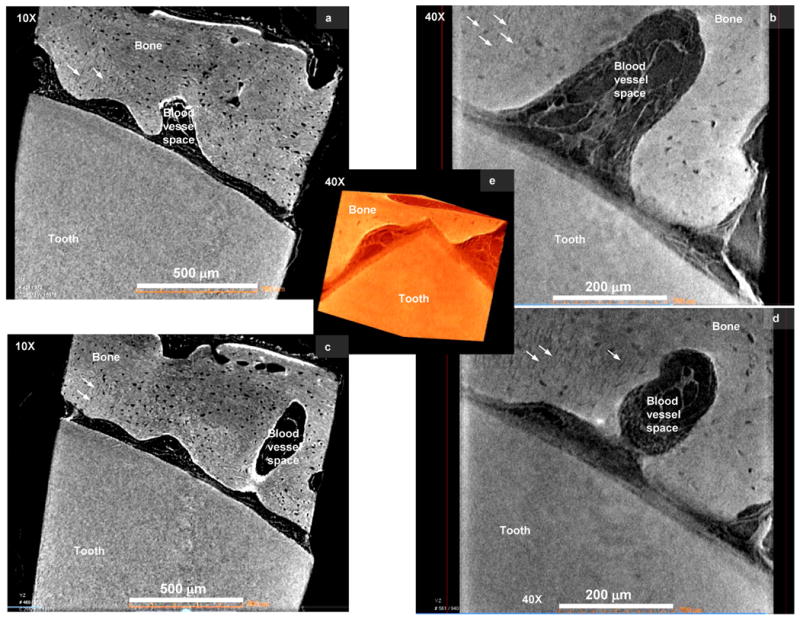
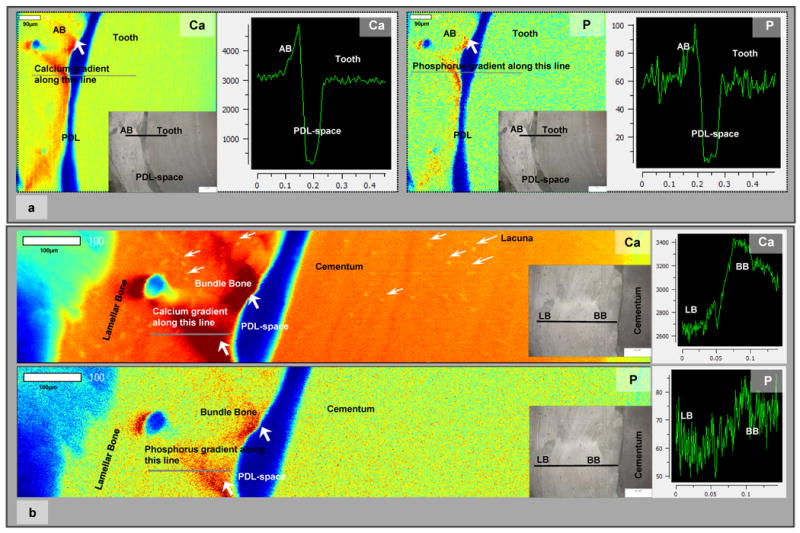
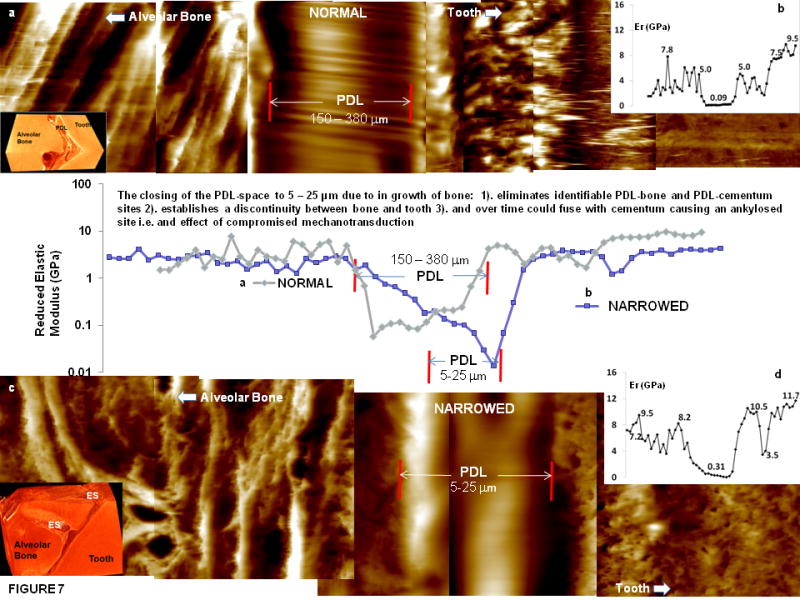
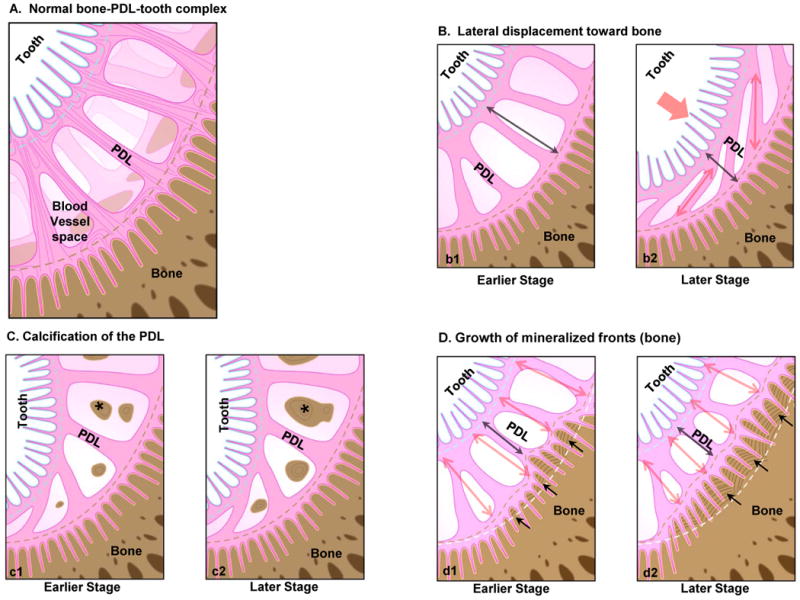
A naturally graded interface due to functional demands can deviate toward a discontinuous interface, eventually decreasing the functional efficiency of a dynamic joint. It is this characteristic feature in a human bone-tooth fibrous joint bone-PDL-tooth complex that will be discussed through histochemistry, and site-specific high resolution microscopy, micro tomography(Micro XCT™), X-ray fluorescence imaging and wet nanoindentation techniques. Results demonstrated two causes for the occurrence of 5-50 μm narrowed PDL-space: 1) microscopic scalloped regions at the PDL-insertion sites and macro-scale stratified layers of bone with rich basophilic lines, and 2) macroscopic bony protrusions. Narrowed PDL-complexes illustrated patchy appearance of asporin, and when imaged under wet conditions using an atomic force microscope (AFM), demonstrated structural reorganization of the PDL, collagen periodicity, organic-dominant areas at the PDL-cementum and PDL-bone entheses and within cementum and bone. Scanning electron microscopy (SEM) results confirmed AFM results. Despite the narrowed PDL, continuity between PDL and vasculature in endosteal spaces of bone was demonstrated using a Micro XCT™. The higher levels of Ca and P X-ray fluorescence using a microprobe were correlated with higher elastic modulus values of 0.1-1.4 and 0.1-1.2 GPa for PDL-bone and PDL-cementum using wet nanoindentation. The ranges in elastic modulus values for PDL-bone and PDL-cementum entheses in 150-380 μm wide PDL-complex were 0.1-1.0 and 0.1-0.6 GPa. Based on these results we propose that strain amplification at the entheses could be minimized with a gradual change in modulus profile, a characteristic of 150-380 μm wide functional PDL-space. However, a discontinuity in modulus profile, a characteristic of 5-50 μm wide narrowed PDL-space would cause compromised mechanotransduction. The constrictions or narrowed sites within the bone-tooth fibrous joint will become the new "load bearing sites" that eventually could cause direct local fusion of bone with cementum.
Published by Elsevier Ltd.
Figures
References
-
- Suresh S. Graded materials for resistance to contact deformation and damage. Science. 2001;292(5526):2447–51. - PubMed
-
- Thompson DAW. On Growth and Form. Cambridge University Press; 1961.
-
- Carter DR, Beaupre GS. Skeletal Function and Form Mechanobiology of Skeletal Development, Aging, and Regeneration. Cambridge University Press; 2001.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
