

DNA/NYVAC vaccine regimen induces HIV-specific CD4 and CD8 T-cell responses in intestinal mucosa
- PMID: 21775454
- PMCID: PMC3196391
- DOI: 10.1128/JVI.00788-11
DNA/NYVAC vaccine regimen induces HIV-specific CD4 and CD8 T-cell responses in intestinal mucosa
Abstract
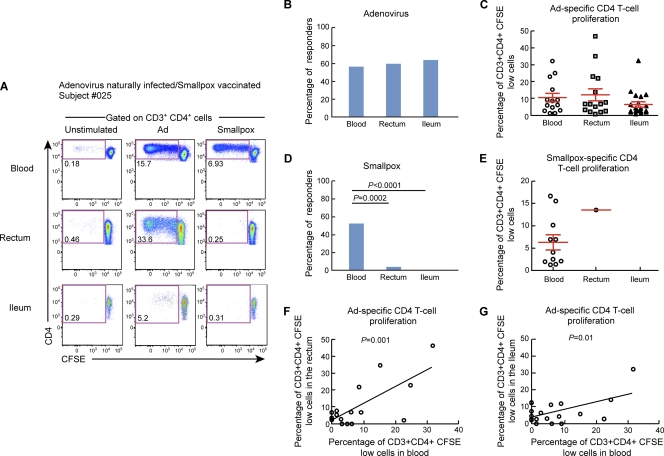
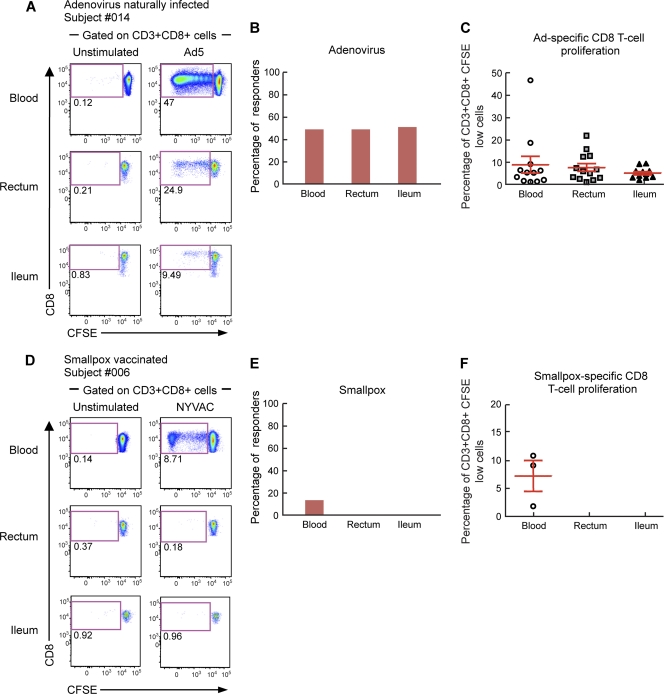
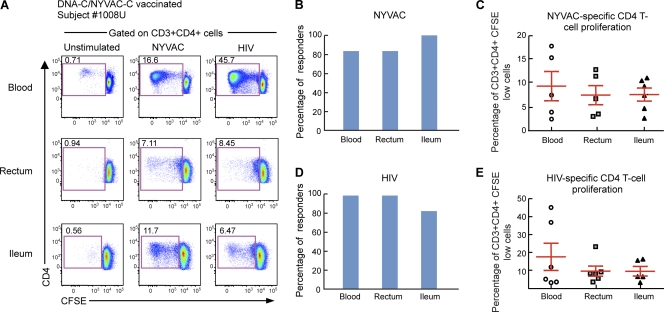
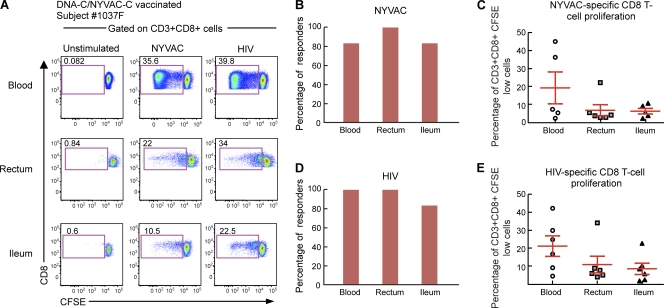
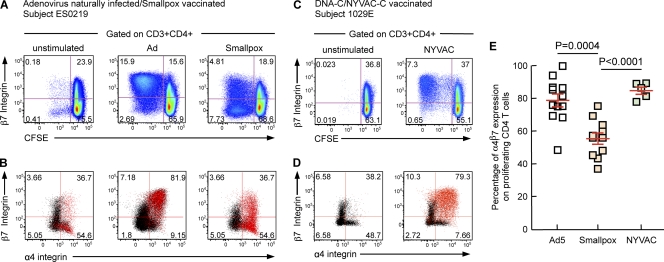
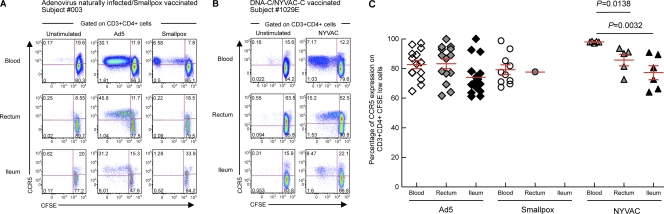
In the present study, we have investigated the anatomic distribution in blood and gut mucosal tissues of memory poxvirus-specific CD4 and CD8 T cells in subjects vaccinated with smallpox and compared it with vector (NYVAC)-specific and HIV insert-specific T-cell responses induced by an experimental DNA-C/ NYVAC-C vaccine regimen. Smallpox-specific CD4 T-cell responses were present in the blood of 52% of the subjects studied, while smallpox-specific CD8 T cells were rarely detected (12%). With one exception, smallpox-specific T cells were not measurable in gut tissues. Interestingly, NYVAC vector-specific and HIV-specific CD4 and CD8 T-cell responses were detected in almost 100% of the subjects immunized with DNA-C/NYVAC-C in blood and gut tissues. The large majority (83%) of NYVAC-specific CD4 T cells expressed α4β7 integrins and the HIV coreceptor CCR5. These results demonstrate that the experimental DNA-C/NYVAC-C HIV vaccine regimen induces the homing of potentially protective HIV-specific CD4 and CD8 T cells in the gut, the port of entry of HIV and one of the major sites for HIV spreading and the depletion of CD4 T cells.
Figures
References
-
- Bart P. A., et al. 2008. EV01: a phase I trial in healthy HIV negative volunteers to evaluate a clade C HIV vaccine, NYVAC-C undertaken by the EuroVacc Consortium. Vaccine 26:3153–3161 - PubMed
-
- Berlin C., et al. 1993. Alpha 4 beta 7 integrin mediates lymphocyte binding to the mucosal vascular addressin MAdCAM-1. Cell 74:185–195 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
