

Electrocardiographic and clinical predictors separating atherosclerotic sudden cardiac death from incident coronary heart disease
- PMID: 21775508
- PMCID: PMC3638973
- DOI: 10.1136/hrt.2010.215871
Electrocardiographic and clinical predictors separating atherosclerotic sudden cardiac death from incident coronary heart disease
Abstract
Objective: To identify specific ECG and clinical predictors that separate atherosclerotic sudden cardiac death (SCD) from incident coronary heart disease (CHD) (non-fatal events and non-sudden death) in the combined cohorts of the Atherosclerosis Risk in Communities study and the Cardiovascular Health Study.
Methods: This analysis included 18,497 participants (58% females, 24% black individuals, mean age 58 years) who were initially free of clinical CHD. A competing risk analysis was conducted to examine the prognostic significance of baseline clinical characteristics and an extensive electronic database of ECG measurements for prediction of 229 cases of SCD as a first event versus 2297 incident CHD cases (2122 non-fatal events and 175 non-sudden death) that occurred during a median follow-up time of 13 years in the Cardiovascular Health Study and 14 years in the Atherosclerosis Risk in Communities study.
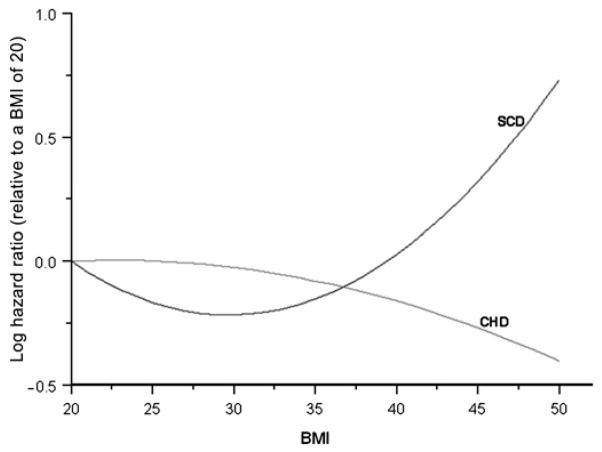
Results: After adjusting for common CHD risk factors, a number of clinical characteristics and ECG measurements were independently predictive of SCD and CHD. However, the risk of SCD versus incident CHD was significantly different for race/ethnicity, hypertension, body mass index (BMI), heart rate, QTc, abnormally inverted T wave in any ECG lead group and level of ST elevation in V2. Black race/ethnicity (compared to non-black) was predictive of high SCD risk but less risk of incident CHD (p value for differences in the risk (HR) for SCD versus CHD <0.0001). Hypertension, increased heart rate, prolongation of QTc and abnormally inverted T wave were stronger predictors of high SCD risk compared to CHD (p value=0.0460, 0.0398, 0.0158 and 0.0265, respectively). BMI was not predictive of incident CHD but was predictive of high SCD risk in a quadratic fashion (p value=0.0220). On the other hand, elevated ST height as measured at the J point and that measured at 60 ms after the J point in V2 were not predictive of SCD but were predictive of high incident CHD risk (p value=0.0251 and 0.0155, respectively).
Conclusions: SCD and CHD have many risk factors in common. Hypertension, race/ethnicity, BMI, heart rate, QTc, abnormally inverted T wave in any ECG lead group and level of ST elevation in V2 have the potential to separate between the risks of SCD and CHD. These results need to be validated in another cohort.
Conflict of interest statement
Figures
References
-
- Sans S, Kesteloot H, Kromhout D. The burden of cardiovascular diseases mortality in Europe. Task Force of the European Society of Cardiology on Cardiovascular Mortality and Morbidity Statistics in Europe. Eur Heart J. 1997;18:1231–48. - PubMed
-
- Nichol G, Aufderheide TP, Eigel B, et al. Regional systems of care for out-of-hospital cardiac arrest: a policy statement from the American Heart Association. Circulation. 2010;121:709–29. - PubMed
-
- Lippert FK, Violetta R, Georgiou M, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 10. The ethics of resuscitation and end-of-life decisions. Resuscitation. 2010;81:1445–51. - PubMed
-
- Hill SF, Sheppard MN. Non-atherosclerotic coronary artery disease associated with sudden death. Heart. 2010;96:1119–25. - PubMed
Publication types
MeSH terms
Grants and funding
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- HHSN268201100009I/HL/NHLBI NIH HHS/United States
- N01-HC-85081/HC/NHLBI NIH HHS/United States
- HHSN268201100011I/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- N01-HC-85082/HC/NHLBI NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- HHSN268201200036C/HL/NHLBI NIH HHS/United States
- N01-HC-55222/HC/NHLBI NIH HHS/United States
- R01-HL-088456/HL/NHLBI NIH HHS/United States
- N01 HC075150/HL/NHLBI NIH HHS/United States
- N01-HC-85084/HC/NHLBI NIH HHS/United States
- N01-HC-85085/HC/NHLBI NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- U01 HL080295/HL/NHLBI NIH HHS/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- HHSN268201100008I/HL/NHLBI NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- N01 HC085086/HL/NHLBI NIH HHS/United States
- R01-HL-087652/HL/NHLBI NIH HHS/United States
- U01-HL-080295/HL/NHLBI NIH HHS/United States
- R01 HL087652/HL/NHLBI NIH HHS/United States
- N01-HC-85086/HC/NHLBI NIH HHS/United States
- R01 HL088456/HL/NHLBI NIH HHS/United States
- N01 HC055222/HL/NHLBI NIH HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- N01 HC085079/HL/NHLBI NIH HHS/United States
- N01-HC-85083/HC/NHLBI NIH HHS/United States
- N01-HC-75150/HC/NHLBI NIH HHS/United States
- N01-HC-85080/HC/NHLBI NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
- HHSN268201100007I/HL/NHLBI NIH HHS/United States
- N01-HC-85079/HC/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases