

Continuous glucose profiles in obese and normal-weight pregnant women on a controlled diet: metabolic determinants of fetal growth
- PMID: 21775754
- PMCID: PMC3177740
- DOI: 10.2337/dc11-0723
Continuous glucose profiles in obese and normal-weight pregnant women on a controlled diet: metabolic determinants of fetal growth
Abstract
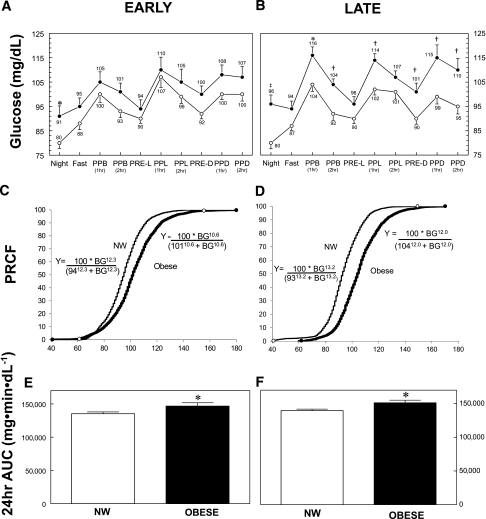
Objective: We sought to define 24-h glycemia in normal-weight and obese pregnant women using continuous glucose monitoring (CGM) while they consumed a habitual and controlled diet both early and late in pregnancy.
Research design and methods: Glycemia was prospectively measured in early (15.7 ± 2.0 weeks' gestation) and late (27.7 ± 1.7 weeks' gestation) pregnancy in normal-weight (n = 22) and obese (n = 16) pregnant women on an ad libitum and controlled diet. Fasting glucose, triglycerides (early pregnancy only), nonesterified fatty acids (FFAs), and insulin also were measured.
Results: The 24-h glucose area under the curve was higher in obese women than in normal-weight women both early and late in pregnancy despite controlled diets. Nearly all fasting and postprandial glycemic parameters were higher in the obese women later in pregnancy, as were fasting insulin, triglycerides, and FFAs. Infants born to obese mothers had greater adiposity. Maternal BMI (r = 0.54, P = 0.01), late average daytime glucose (r = 0.48, P < 0.05), and late fasting insulin (r = 0.49, P < 0.05) correlated with infant percentage body fat. However, early fasting triglycerides (r = 0.67, P < 0.001) and late fasting FFAs (r = 0.54, P < 0.01) were even stronger correlates.
Conclusions: This is the first study to demonstrate that obese women without diabetes have higher daytime and nocturnal glucose profiles than normal-weight women despite a controlled diet both early and late in gestation. Body fat in infants, not birth weight, was related to maternal BMI, glucose, insulin, and FFAs, but triglycerides were the strongest predictor. These metabolic findings may explain higher rates of infant macrosomia in obese women, which might be targeted in trials to prevent excess fetal growth.
Figures

Comment in
-
Aiming at new targets to achieve normoglycemia during pregnancy.Diabetes Care. 2011 Oct;34(10):2331-2. doi: 10.2337/dc11-1411. Diabetes Care. 2011. PMID: 21949225 Free PMC article. No abstract available.
References
-
- American College of Obstetricians and Gynecologists ACOG Committee opinion number 315, September 2005: obesity in pregnancy. Obstet Gynecol 2005;106:671–675 - PubMed
-
- Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM. Prevalence of overweight and obesity in the United States, 1999-2004. JAMA 2006;295:1549–1555 - PubMed
-
- Catalano PM. Management of obesity in pregnancy. Obstet Gynecol 2007;109:419–433 - PubMed
-
- Metzger BE, Lowe LP, Dyer AR, et al. ; HAPO Study Cooperative Research Group Hyperglycemia and adverse pregnancy outcomes. N Engl J Med 2008;358:1991–2002 - PubMed
-
- Metzger BE, Buchanan TA, Coustan DR, et al. Summary and recommendations of the Fifth International Workshop-Conference on Gestational Diabetes Mellitus. Diabetes Care 2007;30(Suppl. 2):S251–S260 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
