

Timing of indicated late-preterm and early-term birth
- PMID: 21775849
- PMCID: PMC3160133
- DOI: 10.1097/AOG.0b013e3182255999
Timing of indicated late-preterm and early-term birth
Abstract
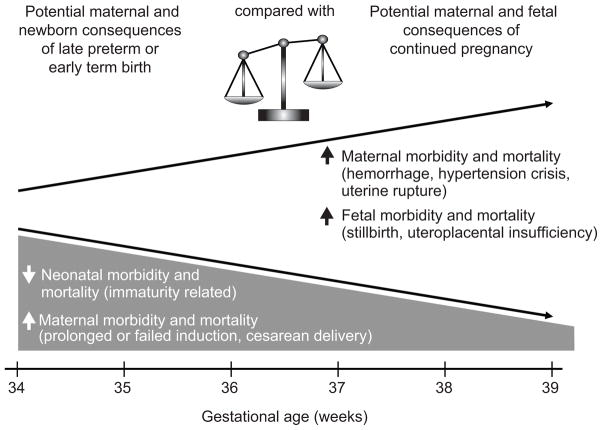
The growing public health awareness of prematurity and its complications has prompted careful evaluation of the timing of deliveries by clinicians and hospitals. Preterm birth is associated with significant morbidity and mortality, and affects more than half a million births in the United States each year. In some situations, however, a late-preterm or early-term birth is the optimal outcome for the mother, child, or both owing to conditions that can result in worse outcomes if pregnancy is allowed to continue. These conditions may be categorized as placental, maternal, or fetal, including conditions such as placenta previa, preeclampsia, and multiple gestations. Some risks associated with early delivery are common to all conditions, including prematurity-related morbidities (eg, respiratory distress syndrome and intraventricular hemorrhage) as well as maternal intrapartum morbidities such as failed induction and cesarean delivery. However, when continuation of the pregnancy is associated with more risks such as hemorrhage, uterine rupture, and stillbirth, preterm delivery maybe indicated. In February 2011, the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the Society for Maternal-Fetal Medicine held a workshop titled "Timing of Indicated Late Preterm and Early Term Births." The goal of the workshop was to synthesize the available information regarding conditions that may result in medically indicated late-preterm and early-term births to determine the potential risks and benefits of delivery compared with continued pregnancy, determine the optimal gestational age for delivery of affected pregnancies when possible, and inform future research regarding these issues. Based on available data and expert opinion, optimal timing for delivery for specific conditions was determined by consensus.
Figures
Comment in
-
Concept of gestational age in "completed weeks": lost in translation.Obstet Gynecol. 2012 Jan;119(1):183-4; author reply 184-5. doi: 10.1097/AOG.0b013e31823ee5d7. Obstet Gynecol. 2012. PMID: 22183232 No abstract available.
References
-
- Raju TN, Higgins RD, Stark AR, Leveno KJ. Optimizing care and outcome for late-preterm (near-term) infants: a summary of the workshop sponsored by the National Institute of Child Health and Human Development. Pediatrics. 2006 Sep;118(3):1207–14. - PubMed
-
- Behrman RE, Butler AS, editors. Committee on understanding premature birth and assuring healthy outcomes, Board on Health Sciences Policy. Institute of Medicine. National Academies Press; 2005. Preterm birth: causes, consequences and prevention. - PubMed
-
- Mathews TH, MacDorman MF. National vital statistics report. 17. Vol. 58. Hyattsville, MD: National Center for Health Statistics; 2010. Infant mortality statistics from the 2006 period linked birth/infant death dataset. - PubMed
-
- Tita AT, Landon MB, Spong CY, Lai Y, Leveno KJ, Varner MW, Moawad AH, Caritis SN, Meis PJ, Wapner RJ, Sorokin Y, Miodovnik M, Carpenter M, Peaceman AM, O’Sullivan MJ, Sibai BM, Langer O, Thorp JM, Ramin SM, Mercer BM Eunice Kennedy Shriver NICHD Maternal-Fetal Medicine Units Network. Timing of elective repeat cesarean delivery at term and neonatal outcomes. N Engl J Med. 2009 Jan 8;360(2):111–20. - PMC - PubMed
-
- Donovan EF, Lannon C, Bailit J, Rose B, Iams JD, Byczkowski T Ohio Perinatal Quality Collaborative Writing Committee. A statewide initiative to reduce inappropriate scheduled births at 36(0/7)-38(6/7) weeks’ gestation. Am J Obstet Gynecol. 2010 Mar;202(3):243.e1–8. Erratum in: Am J Obstet Gynecol. 2010 Jun;202(6):603. - PubMed
