

Seated cuff blood pressure-lowering efficacy of an olmesartan medoxomil-based treatment regimen in patients with type 2 diabetes mellitus
- PMID: 21777013
- PMCID: PMC3585768
- DOI: 10.2165/11592830-000000000-00000
Seated cuff blood pressure-lowering efficacy of an olmesartan medoxomil-based treatment regimen in patients with type 2 diabetes mellitus
Abstract
Background: Hypertension is a common co-morbidity in patients with type 2 diabetes mellitus, and well tolerated, effective therapies are needed to achieve guideline-recommended blood pressure (BP) goals in these patients.
Objective: The aim of this study was to present the results of a prespecified analysis of key secondary endpoints from a 12-week, open-label, single-arm study evaluating the efficacy and safety of olmesartan medoxomil plus hydrochlorothiazide (HCTZ) in patients with hypertension and type 2 diabetes.
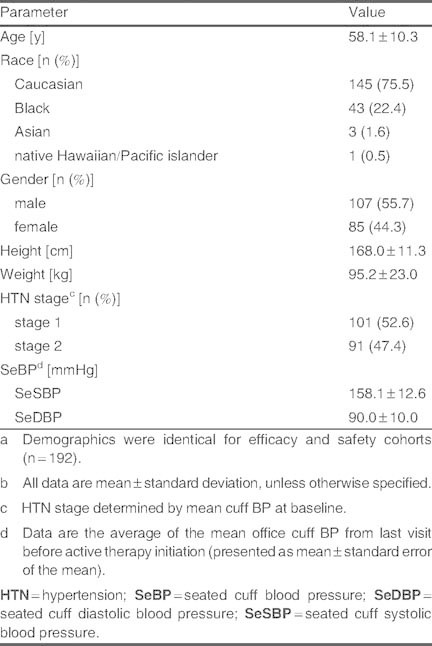
Study design and methods: After a placebo run-in period, 192 patients received olmesartan medoxomil 20 mg/day for 3 weeks. If BP remained ≥ 120/70 mmHg, patients were uptitrated at 3-week intervals to olmesartan medoxomil 40 mg/day, olmesartan medoxomil/HCTZ 40/12.5 mg/day, and olmesartan medoxomil/HCTZ 40/25 mg/day.
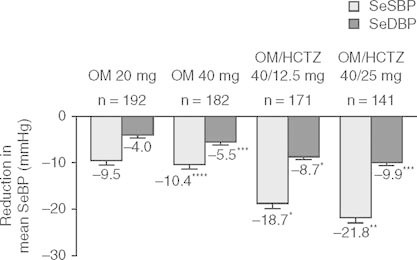
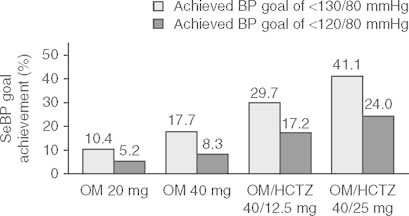
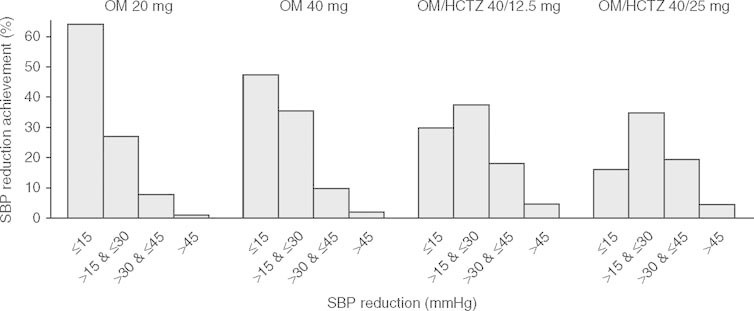
Main outcome measure: Endpoints evaluated in this analysis were the change from baseline in mean seated cuff BP (SeBP), proportions of patients achieving SeBP goals, and distribution of SeBP reductions.
Results: Mean SeBP was 158.1/90.0 mmHg at baseline. The mean ± standard error of BP reductions at 12 weeks for systolic and diastolic BP were 21.3 ± 1.1 mmHg and 9.8 ± 0.6 mmHg, respectively (p < 0.0001 for each). At the end of the study, the proportion of patients with diabetes achieving the recommended SeBP goal of <130/80 mmHg was 41.1%.
Conclusions: An olmesartan medoxomil ± HCTZ treatment regimen significantly reduced BP from baseline in patients with hypertension and type 2 diabetes.
Clinical trials registration: ClinicalTrials.gov identifier: NCT00403481.
Figures
Similar articles
-
Efficacy of olmesartan medoxomil and hydrochlorothiazide fixed-dose combination therapy in patients aged 65 years and older with stage 1 and 2 hypertension or isolated systolic hypertension.Am J Cardiovasc Drugs. 2012 Oct 1;12(5):325-33. doi: 10.1007/BF03261841. Am J Cardiovasc Drugs. 2012. PMID: 22920048 Clinical Trial.
-
Safety and tolerability of an olmesartan medoxomil-based regimen in patients with stage 1 hypertension: a randomized, double-blind, placebo-controlled study.Clin Drug Investig. 2010;30(7):473-82. doi: 10.2165/11536560-000000000-00000. Clin Drug Investig. 2010. PMID: 20528002 Clinical Trial.
-
Blood pressure-lowering efficacy of an olmesartan medoxomil/hydrochlorothiazide-based treatment algorithm in elderly patients (age ≥65 years) stratified by age, sex and race: subgroup analysis of a 12-week, open-label, single-arm, dose-titration study.Drugs Aging. 2011 Jun 1;28(6):477-90. doi: 10.2165/11589460-000000000-00000. Drugs Aging. 2011. PMID: 21639407 Clinical Trial.
-
Olmesartan medoxomil/amlodipine/hydrochlorothiazide: fixed-dose combination in hypertension.Drugs. 2011 Jan 22;71(2):209-20. doi: 10.2165/11206770-000000000-00000. Drugs. 2011. PMID: 21275446 Review.
-
Olmesartan medoxomil combined with hydrochlorothiazide for the treatment of hypertension.Vasc Health Risk Manag. 2006;2(4):401-9. doi: 10.2147/vhrm.2006.2.4.401. Vasc Health Risk Manag. 2006. PMID: 17323594 Free PMC article. Review.
Cited by
-
Integrated control of hypertension by olmesartan medoxomil and hydrochlorothiazide and rationale for combination.Integr Blood Press Control. 2011;4:73-83. doi: 10.2147/IBPC.S12214. Epub 2011 Dec 7. Integr Blood Press Control. 2011. PMID: 22253546 Free PMC article.
-
Safety, tolerability, and efficacy of a fixed-dose combination of olmesartan 40 mg and hydrochlorothiazide 12.5/25 mg in daily practice.Vasc Health Risk Manag. 2013;9:475-83. doi: 10.2147/VHRM.S49118. Epub 2013 Aug 26. Vasc Health Risk Manag. 2013. PMID: 24039432 Free PMC article.
References
-
- Arauz-Pacheco C, Parrott MA, Raskin P. Hypertension management in adults with diabetes. Diabetes Care. 2004;27(Suppl.1):65–7. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical