

Acute chest pain - a prospective population based study of contacts to Norwegian emergency medical communication centres
- PMID: 21777448
- PMCID: PMC3155474
- DOI: 10.1186/1471-227X-11-9
Acute chest pain - a prospective population based study of contacts to Norwegian emergency medical communication centres
Abstract
Background: Acute chest pain is a frequently occurring symptom in patients with medical emergencies and imposes potentially life threatening situations outside hospitals. Little is known about the epidemiology of patients with acute chest pain in a primary care setting in Norway, and we aimed to obtain more representative data on such patients using data from emergency medical communication centres (EMCCs).
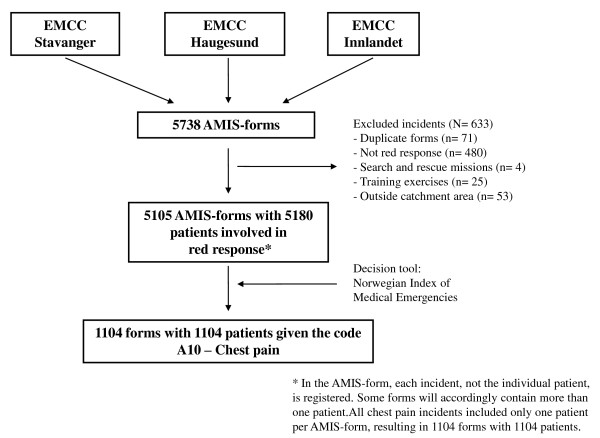
Methods: Data were collected prospectively during three months in 2007 from three EMCCs, covering 816 000 inhabitants. The EMCCs gathered information on every situation that was triaged as a red response (defined as an "acute" response, with the highest priority), according to the Norwegian Index of Medical Emergencies. Records from ambulances and primary care doctors were subsequently collected. International Classification of Primary Care - 2 symptom codes and The National Committee on Aeronautics (NACA) System scores were assigned retrospectively. Only chest pain patients were included in the study.
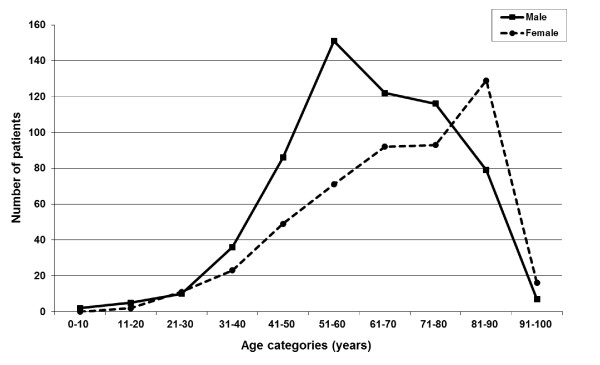
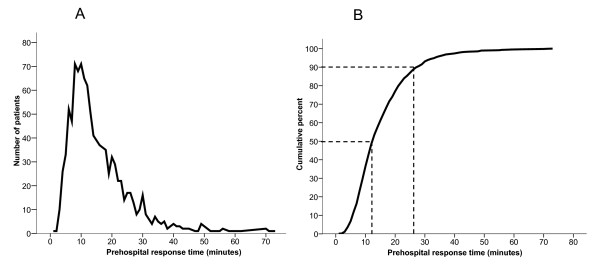
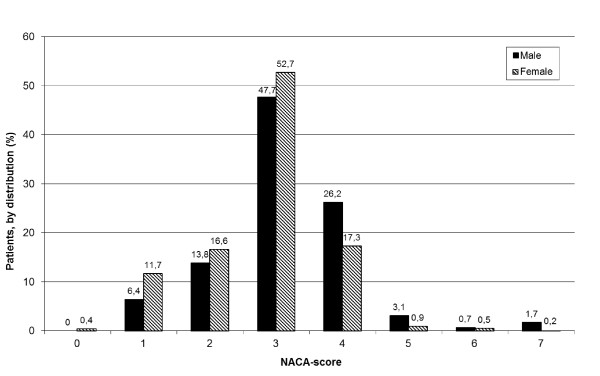
Results: 5 180 patients were involved in red response situations, of which 21% had chest pain. Estimated rate was 5.4 chest pain cases per 1000 inhabitants per year. NACA-scores indicated that 26% of the patients were in a life-threatening medical situation. Median prehospital response time was 13 minutes; an ambulance reached the patient in less than 10 minutes in 30% of the cases. Seventy-six per cent of the patients with chest pain were admitted to a hospital for further investigation, 14% received final treatment at a casualty clinic, while 10% had no further investigation by a doctor ("left at the scene").
Conclusions: The majority of patients with acute chest pain were admitted to a hospital for further investigation, but only a quarter of the patients were assessed prehospitally to have a severe illness. This sheds light on the challenges for the EMCCs in deciding the appropriate level of response in patients with acute chest pain. Overtriage is to some extent both expected and desirable to intercept all patients in need of immediate help, but it is also well known that overtriage is resource demanding. Further research is needed to elucidate the challenges in the diagnosis and management of chest pain outside hospitals.
Figures
References
-
- Deakin CD, Sherwood DM, Smith A. et al.Does telephone triage of emergency (999) calls using Advanced Medical Priority Dispatch (AMPDS) with Department of Health (DH) call prioritisation effectively identify patients with an acute coronary syndrome? An audit of 42,657 emergency calls to Hampshire Ambulance Service NHS Trust. Emerg Med J. 2006;23(3):232–5. doi: 10.1136/emj.2004.022962. - DOI - PMC - PubMed
-
- Cayley WE Jr. Diagnosing the cause of chest pain. Am Fam Physician. 2005;72(10):2012–21. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
