

Reactive glia not only associates with plaques but also parallels tangles in Alzheimer's disease
- PMID: 21777559
- PMCID: PMC3157187
- DOI: 10.1016/j.ajpath.2011.05.047
Reactive glia not only associates with plaques but also parallels tangles in Alzheimer's disease
Abstract
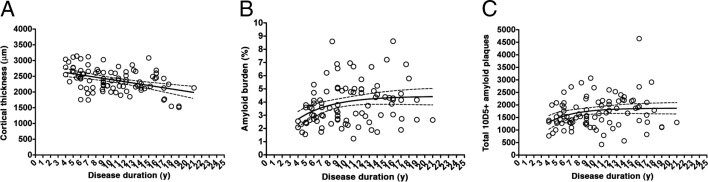
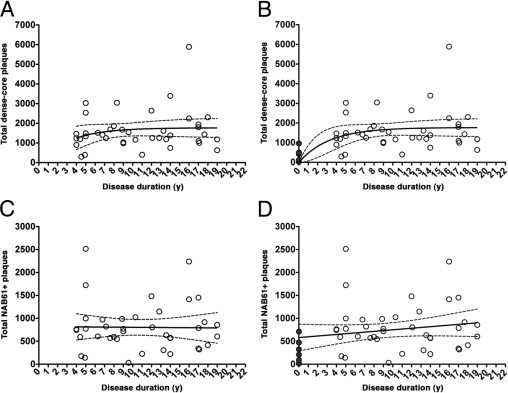
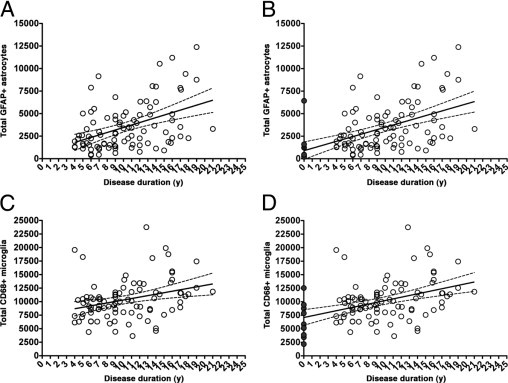
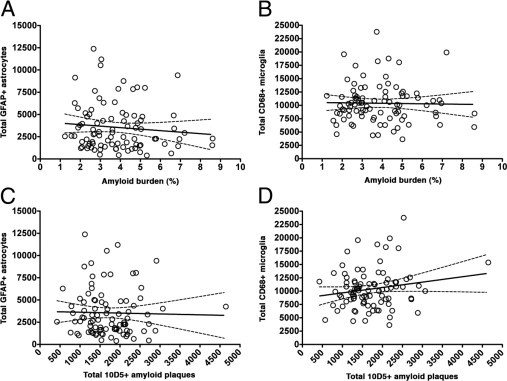
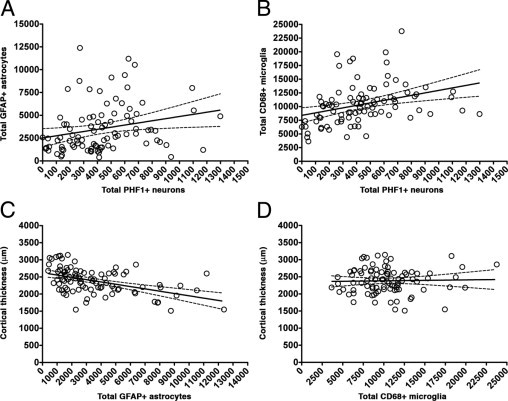
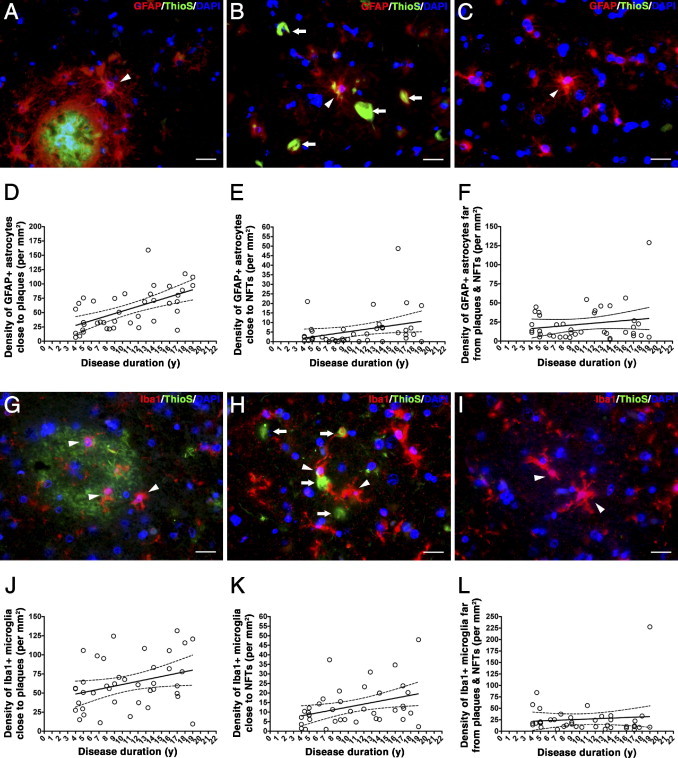
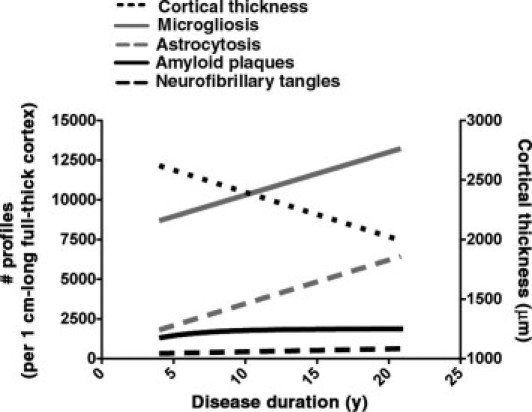
Senile plaques are a prominent pathological feature of Alzheimer's disease (AD), but little is understood about the association of glial cells with plaques or about the dynamics of glial responses through the disease course. We investigated the progression of reactive glial cells and their relationship with AD pathological hallmarks to test whether glial cells are linked only to amyloid deposits or also to tangle deposition, thus integrating both lesions as a marker of disease severity. We conducted a quantitative stereology-based post-mortem study on the temporal neocortex of 15 control subjects without dementia and 91 patients with AD, including measures of amyloid load, neurofibrillary tangles, reactive astrocytes, and activated microglia. We also addressed the progression of glial responses in the vicinity (≤50 μm) of dense-core plaques and tangles. Although the amyloid load reached a plateau early after symptom onset, astrocytosis and microgliosis increased linearly throughout the disease course. Moreover, glial responses correlated positively with tangle burden, whereas astrocytosis correlated negatively with cortical thickness. However, neither correlated with amyloid load. Glial responses increased linearly around existing plaques and in the vicinity of tangles. These results indicate that the progression of astrocytosis and microgliosis diverges from that of amyloid deposition, arguing against a straightforward relationship between glial cells and plaques. They also suggest that reactive glia might contribute to the ongoing neurodegeneration.
Copyright © 2011 American Society for Investigative Pathology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Itagaki S., McGeer P.L., Akiyama H., Zhu S., Selkoe D. Relationship of microglia and astrocytes to amyloid deposits of Alzheimer disease. J Neuroimmunol. 1989;24:173–182. - PubMed
-
- Ingelsson M., Fukumoto H., Newell K.L., Growdon J.H., Hedley-Whyte E.T., Frosch M.P., Albert M.S., Hyman B.T., Irizarry M.C. Early Aβ accumulation and progressive synaptic loss, gliosis, and tangle formation in AD brain. Neurology. 2004;62:925–931. - PubMed
-
- McKhann G., Drachman D., Folstein M., Katzman R., Price D., Stadlan E.M. Clinical diagnosis of Alzheimer's disease: report of the NINCDS-ADRDA Work Group under the auspices of the Department of Health and Human Services Task Force on Alzheimer's Disease. Neurology. 1984;34:939–944. - PubMed
-
- The National Institute on Aging, and Reagan Institute Working Group on Diagnostic Criteria for the Neuropathological Assessment of Alzheimer's Disease: Consensus recommendations for the postmortem diagnosis of Alzheimer's disease. Neurobiol Aging. 1997;18(Suppl):S1–S2. - PubMed
-
- Freeman S.H., Kandel R., Cruz L., Rozkalne A., Newell K., Frosch M.P., Hedley-Whyte E.T., Locascio J.J., Lipsitz L.A., Hyman B.T. Preservation of neuronal number despite age-related cortical brain atrophy in elderly subjects without Alzheimer disease. J Neuropathol Exp Neurol. 2008;67:1205–1212. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
