

A brief screening tool for assessing psychological trauma in clinical practice: development and validation of the New York PTSD Risk Score
- PMID: 21777981
- PMCID: PMC3557518
- DOI: 10.1016/j.genhosppsych.2011.06.001
A brief screening tool for assessing psychological trauma in clinical practice: development and validation of the New York PTSD Risk Score
Abstract
Objective: The objective was to develop a brief posttraumatic stress disorder (PTSD) screening instrument that is useful in clinical practice, similar to the Framingham Risk Score used in cardiovascular medicine.
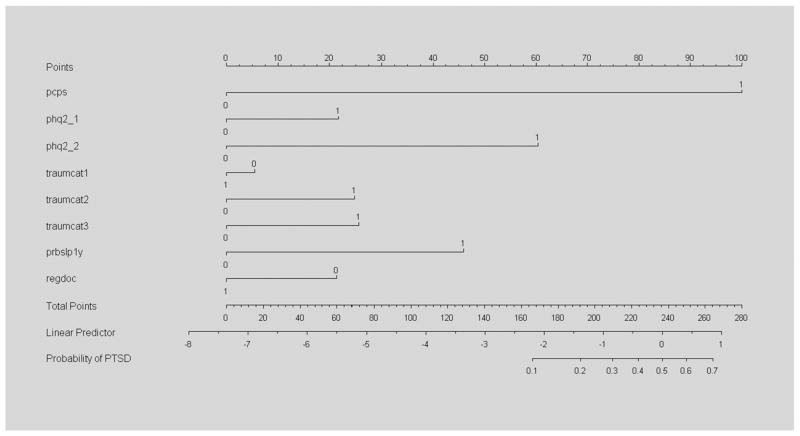
Methods: We used data collected in New York City after the World Trade Center disaster (WTCD) and other trauma data to develop a new PTSD prediction tool--the New York PTSD Risk Score. We used diagnostic test methods to examine different clinical domains, including PTSD symptoms, trauma exposures, sleep disturbances, suicidal thoughts, depression symptoms, demographic factors and other measures to assess different PTSD prediction models.
Results: Using receiver operating curve (ROC) and bootstrap methods, five prediction domains, including core PTSD symptoms, sleep disturbance, access to care status, depression symptoms and trauma history, and five demographic variables, including gender, age, education, race and ethnicity, were identified. For the best prediction model, the area under the ROC curve (AUC) was 0.880 for the Primary Care PTSD Screen alone (specificity=82.2%, sensitivity=93.7%). Adding care status, sleep disturbance, depression and trauma exposure increased the AUC to 0.943 (specificity=85.7%, sensitivity=93.1%), a significant ROC improvement (P<.0001). Adding demographic variables increased the AUC to 0.945, which was not significant (P=.250). To externally validate these models, we applied the WTCD results to 705 pain patients treated at a multispecialty group practice and to 225 trauma patients treated at a Level I Trauma Center. These results validated those from the original WTCD development and validation samples.
Conclusion: The New York PTSD Risk Score is a multifactor prediction tool that includes the Primary Care PTSD Screen, depression symptoms, access to care, sleep disturbance, trauma history and demographic variables and appears to be effective in predicting PTSD among patients seen in healthcare settings. This prediction tool is simple to administer and appears to outperform other screening measures.
Copyright © 2011 Elsevier Inc. All rights reserved.
Figures
Comment in
-
The New York PTSD risk score predicts having, not developing, PTSD.Gen Hosp Psychiatry. 2012 May-Jun;34(3):317. doi: 10.1016/j.genhosppsych.2012.01.003. Epub 2012 Feb 2. Gen Hosp Psychiatry. 2012. PMID: 22305366 No abstract available.
Similar articles
-
PTSD onset and course following the World Trade Center disaster: findings and implications for future research.Soc Psychiatry Psychiatr Epidemiol. 2009 Oct;44(10):887-98. doi: 10.1007/s00127-009-0011-y. Epub 2009 Mar 7. Soc Psychiatry Psychiatr Epidemiol. 2009. PMID: 19277439 Free PMC article.
-
The New York PTSD risk score for assessment of psychological trauma: male and female versions.Psychiatry Res. 2012 Dec 30;200(2-3):827-34. doi: 10.1016/j.psychres.2012.04.022. Epub 2012 May 29. Psychiatry Res. 2012. PMID: 22648009 Free PMC article.
-
Predicting Future PTSD using a Modified New York Risk Score: Implications for Patient Screening and Management.Minerva Psichiatr. 2012 Mar;53(1):47-59. Minerva Psichiatr. 2012. PMID: 22408285 Free PMC article.
-
[Posttraumatic stress disorder (PTSD) as a consequence of the interaction between an individual genetic susceptibility, a traumatogenic event and a social context].Encephale. 2012 Oct;38(5):373-80. doi: 10.1016/j.encep.2011.12.003. Epub 2012 Jan 24. Encephale. 2012. PMID: 23062450 Review. French.
-
Best practices for managing depression and suicide risk in World Trade Center responders and survivors.Arch Environ Occup Health. 2023;78(4):244-248. doi: 10.1080/19338244.2023.2201879. Epub 2023 May 31. Arch Environ Occup Health. 2023. PMID: 37254914 Review.
Cited by
-
Development and preliminary performance of a risk factor screen to predict posttraumatic psychological disorder after trauma exposure.Gen Hosp Psychiatry. 2017 May;46:25-31. doi: 10.1016/j.genhosppsych.2016.12.011. Epub 2016 Dec 27. Gen Hosp Psychiatry. 2017. PMID: 28622811 Free PMC article.
-
Prevalence and correlates of substance use among trans female youth ages 16-24 years in the San Francisco Bay Area.Drug Alcohol Depend. 2015 Feb 1;147:160-6. doi: 10.1016/j.drugalcdep.2014.11.023. Epub 2014 Dec 15. Drug Alcohol Depend. 2015. PMID: 25548025 Free PMC article.
-
The Impact of Discrimination on the Mental Health of Trans*Female Youth and the Protective Effect of Parental Support.AIDS Behav. 2016 Oct;20(10):2203-2211. doi: 10.1007/s10461-016-1409-7. AIDS Behav. 2016. PMID: 27115401 Free PMC article.
-
Use of the New York PTSD risk score to predict PTSD: current and future research efforts.Gen Hosp Psychiatry. 2012 May-Jun;34(3):317-9. doi: 10.1016/j.genhosppsych.2012.01.005. Epub 2012 Feb 9. Gen Hosp Psychiatry. 2012. PMID: 22325632 Free PMC article. No abstract available.
-
Deconvolution of Transcriptional Networks in Post-Traumatic Stress Disorder Uncovers Master Regulators Driving Innate Immune System Function.Sci Rep. 2017 Nov 3;7(1):14486. doi: 10.1038/s41598-017-15221-y. Sci Rep. 2017. PMID: 29101382 Free PMC article.
References
-
- Haynes RB, Sackett DL, Guyatt GH, Tugwell P. Clinical epidemiology: how to do clinical practice research. 3. New York: Lippincott Williams & Wilkins; 2006. pp. 273–322.
-
- Fauci AS, Braunwald E, Kasper DL, Hauser SL, editors. Harrison’s principles of internal medicine. 17. New York: McGraw–Hill; 2008. pp. 26–8.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
