

doi: 10.1155/2011/231493.
Epub 2011 Jul 12.
Perioperative intravascular fluid assessment and monitoring: a narrative review of established and emerging techniques
Affiliations
- PMID: 21785588
- PMCID: PMC3139886
- DOI: 10.1155/2011/231493
Item in Clipboard
Perioperative intravascular fluid assessment and monitoring: a narrative review of established and emerging techniques
Anesthesiol Res Pract.
2011.
Abstract
Accurate assessments of intravascular fluid status are an essential part of perioperative care and necessary in the management of the hemodynamically unstable patient. Goal-directed fluid management can facilitate resuscitation of the hypovolemic patient, reduce the risk of fluid overload, reduce the risk of the injudicious use of vasopressors and inotropes, and improve clinical outcomes. In this paper, we discuss the strengths and limitations of a spectrum of noninvasive and invasive techniques for assessing and monitoring intravascular volume status and fluid responsiveness in the perioperative and critically ill patient.
Figures
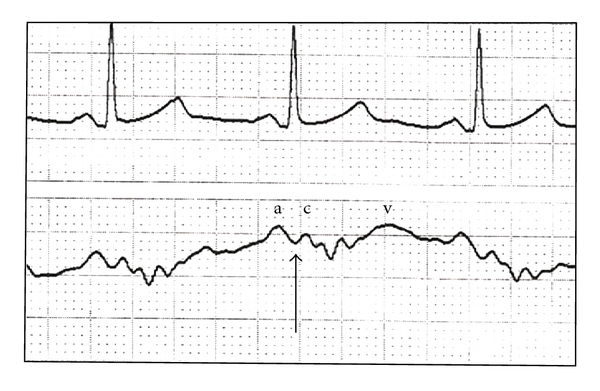
A typical CVP waveform (lower tracing) and accompanying electrocardiogram (upper). The a, c, and v waves are shown, along with the z point (arrow), indicating the appropriate time in the cardiac cycle for CVP measurement. All analyses need to occur at end expiration.
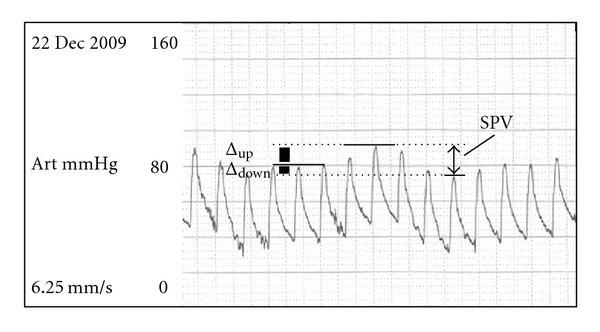
Arterial line tracings showing systolic pressure variation during the respiratory cycle. The pressure at end expiration defines baseline systolic pressure. SPV has two components, delta up and delta down, corresponding to systolic pressure waves reading at peak amplitude of early inspiration (the upward component or delta up) and at end inspiration (the downward component or delta down). The total amplitude variation or the sum of delta up and delta down is thus the SPV, shown with the arrow on the right of the diagram.
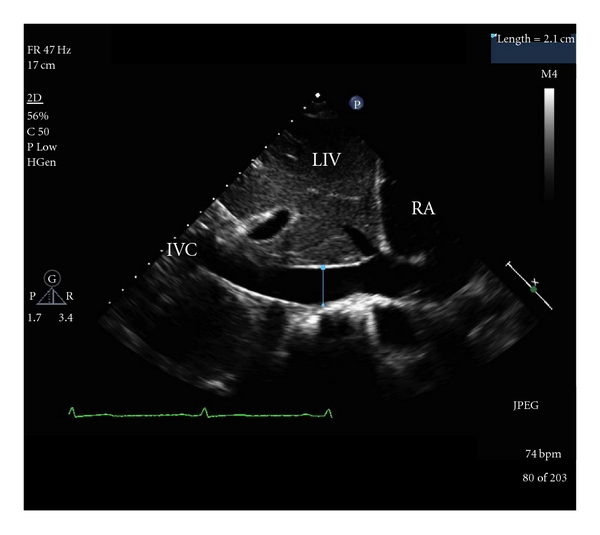
A subcostal view of the cavoatrial junction and adjacent structures. RA: right atrium; IVC: inferior vena cava; LIV: liver.
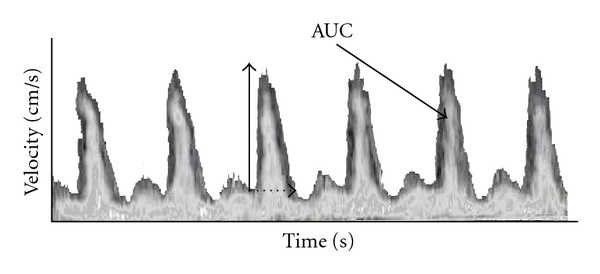
Esophageal Doppler tracings from descending aorta blood flow. Flow time and peak velocity are indicated by dashed and vertical arrows, respectively. Parameters derived from the latter measurements include corrected flow time (FTc), acceleration, and stroke distance. The area under the curve (AUC) is equivalent to stroke distance, the length traveled by an erythrocyte during a single cardiac cycle. Assuming that the flow is via a cylindrical path, the stroke volume (SV) is the product of aortic cross-sectional area and the stroke distance. Aortic blood flow is calculated from the product of heart rate and calculated SV and is not exactly equal to true cardiac output, as approximately 10% of total cardiac output is diverted to subclavian and cerebral arteries upstream to where flow is measured.
References
-
- Jabot J, Teboul JL, Richard C, Monnet X. Passive leg raising for predicting fluid responsiveness: importance of the postural change. Intensive Care Medicine. 2009;35(1):85–90. - PubMed
-
- Préau S, Saulnier F, Dewavrin F, Durocher A, Chagnon JL. Passive leg raising is predictive of fluid responsiveness in spontaneously breathing patients with severe sepsis or acute pancreatitis. Critical Care Medicine. 2010;38(3):819–825. - PubMed
-
- Lamia B, Ochagavia A, Monnet X, Chemla D, Richard C, Teboul JL. Echocardiographic prediction of volume responsiveness in critically ill patients with spontaneously breathing activity. Intensive Care Medicine. 2007;33(7):1125–1132. - PubMed
-
- Monnet X, Rienzo M, Osman D, et al. Passive leg raising predicts fluid responsiveness in the critically ill. Critical Care Medicine. 2006;34(5):1402–1407. - PubMed
-
- Boldt J, Lenz M, Kumle B, Papsdorf M. Volume replacement strategies on intensive care units: results from a postal survey. Intensive Care Medicine. 1998;24(2):147–151. - PubMed
LinkOut - more resources
Full Text Sources
