

TREATMENT AND SURVIVAL PATTERNS IN RELATION TO MULTIMORBIDITY IN PATIENTS WITH LOCOREGIONAL BREAST AND COLORECTAL CANCER
- PMID: 21785664
- PMCID: PMC3140210
- DOI: 10.1016/j.jgo.2011.02.004
TREATMENT AND SURVIVAL PATTERNS IN RELATION TO MULTIMORBIDITY IN PATIENTS WITH LOCOREGIONAL BREAST AND COLORECTAL CANCER
Abstract
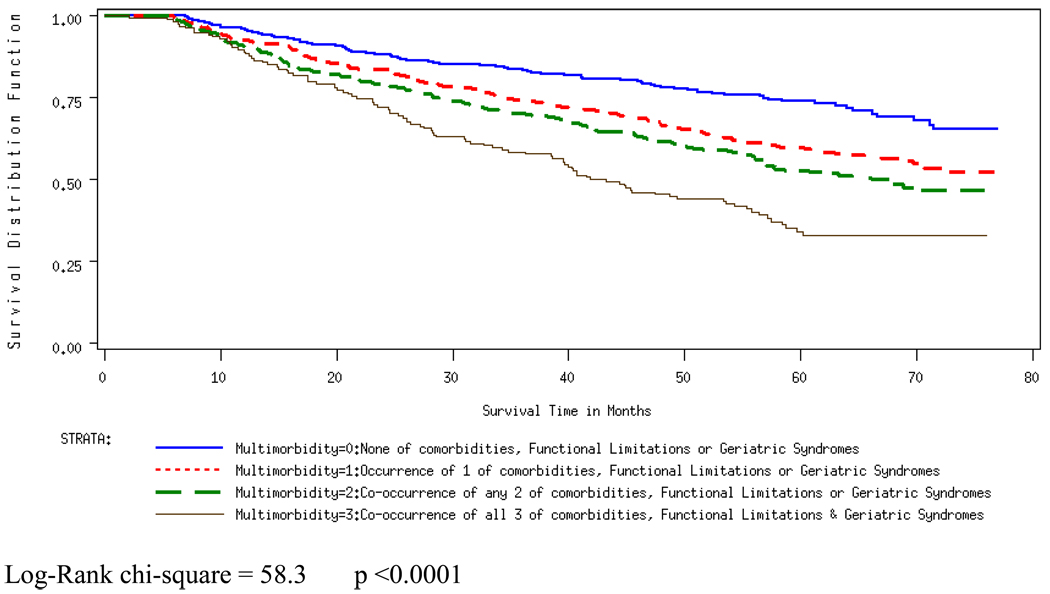
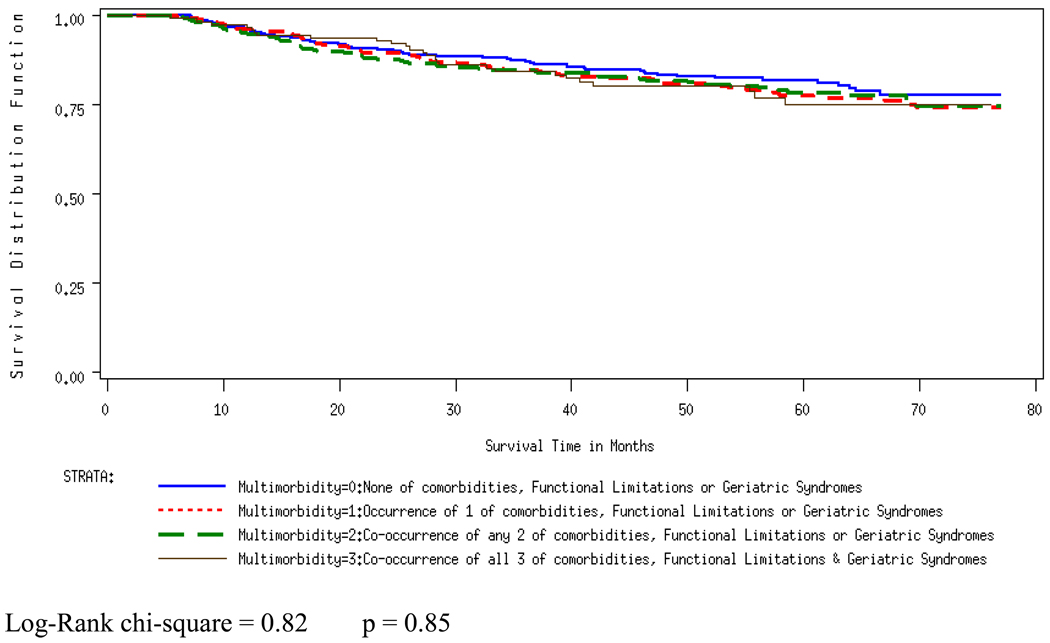
PURPOSE: To examine the effects of the occurrence and co-occurrence of comorbidities (COM), functional limitations (FL), and geriatric syndromes (GS) on treatment and outcomes in older cancer patients. MATERIALS AND METHODS: We used records from the Ohio Cancer Incidence Surveillance System linked with Medicare data, clinical assessment data from the home health care Outcomes and Assessment Information Set, and death certificate data. Our patient population included fee-for-service HHC Medicare beneficiaries diagnosed with incident loco-regional breast or colorectal cancer in years 1999-2001 (n=1236). We grouped patients according to the presence of multimorbidity: (0): none of COM, FL, or GS; (1): occurrence - but no co-occurrence - of COM, FL, or GS; (2): co-occurrence of any two of COM, FL, and GS; and (3): co-occurrence of all three of COM, FL, and GS. Our outcomes were receipt of standard treatment, as well as overall survival (OS) and disease-specific survival (DSS) through 2005. Multivariable regression models were developed to analyze the independent association between multimorbidity and the outcomes, before and after adjusting for age. RESULTS: The effect of multimorbidity on our outcomes was attenuated considerably by age. Adjusting for age and compared with no multimorbidity (0), high multimorbidity (3) remained significantly and negatively associated with receipt of standard treatment (adjusted odds ratio: 0.57, 95% Confidence Interval (CI): 0.33, 0.97). Furthermore, high multimorbidity (3) was associated with increased hazard for OS, but not for DSS (adjusted hazard ratio and 95% CI: 2.15 (1.58, 2.93) for three entities). CONCLUSION: Multimorbidity is significantly and independently associated with cancer treatment and OS, but not DSS.
Figures
References
-
- Satariano WA, Silliman RA. Comorbidity: implications for research and practice in geriatric oncology. Crit Rev Oncol Hematol. 2003 Nov;48(2):239–248. - PubMed
-
- Yates JW. Comorbidity considerations in geriatric oncology research. CA Cancer J Clin. 2001 Nov-Dec;51(6):329–336. - PubMed
-
- Balducci L. Aging, frailty, and chemotherapy. Cancer Control. 2007 Jan;14(1):7–12. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources