

Adjacent segment degeneration after instrumented posterolateral lumbar fusion: a prospective cohort study with a minimum five-year follow-up
- PMID: 21786038
- PMCID: PMC3207344
- DOI: 10.1007/s00586-011-1917-0
Adjacent segment degeneration after instrumented posterolateral lumbar fusion: a prospective cohort study with a minimum five-year follow-up
Abstract
Purpose: To (1) clarify the role of various risk factors in the development of ASD, (2) compare instrumentation configuration with the development of ASD, (3) correlate the radiological incidence of ASD and its clinical outcome and (4) compare the clinical outcome between patients with radiological evidence of ASD and without ASD.
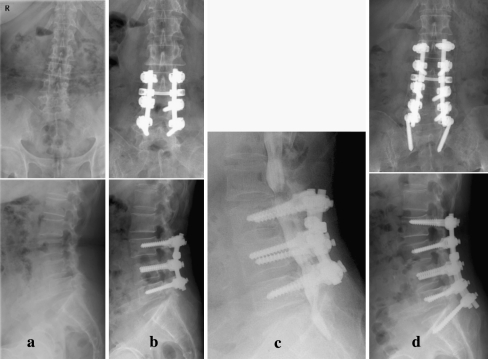
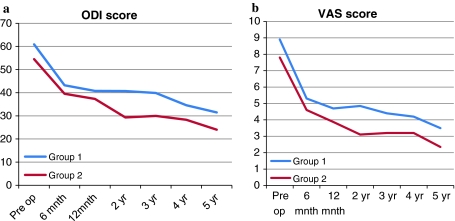
Methods: This study prospectively examined 74 consecutive patients who underwent instrumented lumbar/lumbosacral fusion for degenerative disease with a minimum follow-up of 5 years. Among the patients, 68 were enrolled in the study. All of the patients had undergone preoperative radiological assessment and postoperative radiological assessment at regular intervals. The onset and progression of ASD changes were evaluated. The patients were divided in two groups: patients with radiographic evidence of ASD (group 1) and patients without ASD changes (group 2). Comprehensive analysis of various risk factors between group 1 and group 2 patients was performed. The Visual Analog Scale (VAS) was used to evaluate the clinical outcome and the functional outcome was evaluated using the Oswestry Disability Index (ODI) before and after surgery along with radiological assessment.
Results: Radiographic ASD occurred in 20.6% (14/68) of patients. Preoperative disc degeneration at an adjacent segment was a significant risk factor for ASD. Other risk factors such as the age of a patient at the time of surgery, gender, preoperative diagnosis, length of fusion, instrumentation configuration, sagittal alignment and lumbar or lumbosacral fusion were not significant risk factors for the development of ASD. There was no correlation between ASD and its clinical outcome as determined at the final follow-up session. In addition, clinical outcome of patients with ASD and without ASD were not comparable.
Conclusions: Patients with preoperative disc degeneration at an adjacent segment were more at risk for the development of ASD. Other risk factors including instrumentation configuration were not significantly associated with ASD. There was no correlation between both the radiological development of ASD and its clinical outcome and the clinical outcome of patients with and without ASD.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
