

Cardiac involvement in Wegener's granulomatosis resistant to induction therapy
- PMID: 21786089
- PMCID: PMC3184393
- DOI: 10.1007/s00330-011-2203-6
Cardiac involvement in Wegener's granulomatosis resistant to induction therapy
Abstract
Objectives: The aim of the study was to assess cardiac involvement in patients with Wegener's granulomatosis (WG), who failed to achieve remission following >6 months induction therapy for life or organ threatening disease.
Methods: Eleven WG patients (eight males, mean age 47 ± 13 years), who failed to achieve remission despite >6 months induction therapy, underwent transthoracic echocardiography (TTE) and cardiac magnetic resonance (CMR).
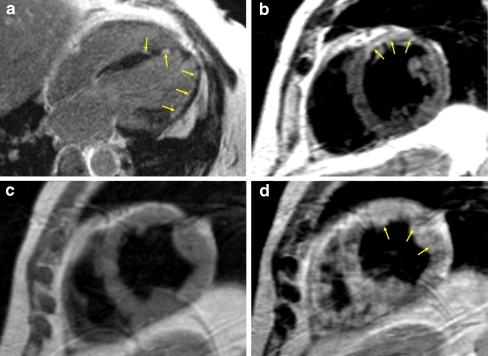
Results: Cardiac involvement was present in 9 (82%) patients. Regional wall motion abnormalities were found in two individuals, but none had left ventricular (LV) ejection fraction <50%. Nine patients had late gadolinium enhancement (LGE) lesions involving LV myocardium and right ventricle free wall was involved in four patients. LGE lesions were found in subepicardial, midwall and subendocardial LV myocardial layers. CMR revealed myocarditis in six patients. Patients with myocarditis had a higher number of LV segments with LGE (5.2 ± 3.4 vs 1.0 ± 1.2, p = 0.03) and more frequent diastolic dysfunction by TTE (5 vs 0, p = 0.02) than those without. Pericardial effusion was observed in five patients, while localized pericardial thickening in six patients.
Conclusions: In WG resistant to >6 months induction therapy cardiac involvement is frequent and is characterized by foci of LGE lesions and signs of myocardial inflammatory process.
Figures
References
-
- Hoffman GS, Kerr GS, Leavitt RY, Hallahan CW, Lebovics RS, Travis WD, Rottem M, Fauci AS. Wegener granulomatosis: an analysis of 158 patients. Ann Intern Med. 1992;116:488–498. - PubMed
-
- Mavrogeni S, Manoussakis MN, Karagiorga TC, Douskou M, Panagiotakos D, Bournia V, Cokkinos DV, Moutsopoulos HM. Detection of coronary artery lesions and myocardial necrosis by magnetic resonance in systemic necrotizing vasculitides. Arthritis Rheum. 2009;61:1121–1129. doi: 10.1002/art.24695. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
