

Prospective, longitudinal study of plastic bronchitis cast pathology and responsiveness to tissue plasminogen activator
- PMID: 21786171
- PMCID: PMC3207025
- DOI: 10.1007/s00246-011-0058-x
Prospective, longitudinal study of plastic bronchitis cast pathology and responsiveness to tissue plasminogen activator
Abstract
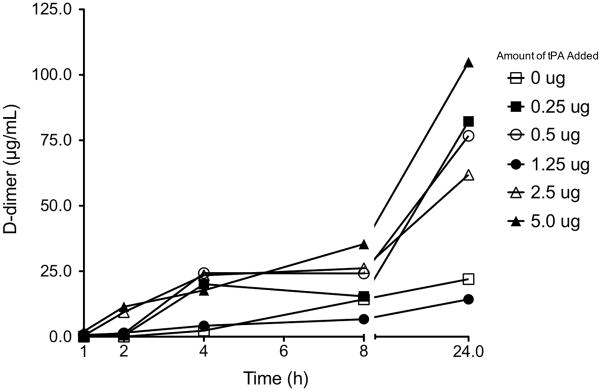
Plastic bronchitis (PB) is a rare disease that often occurs in patients with congenital heart disease (CHD) who have undergone staged single-ventricle palliation. It is characterized by the formation of rubbery "casts" in the airways. PB treatment frequently includes inhaled tissue plasminogen activator (tPA). However, the efficacy of tPA to reduce cast burden is unknown. This is further complicated by our lack of knowledge of cast composition. We obtained spontaneously expectorated PB casts from children (n = 4) with CHD and one adult patient with idiopathic PB. Pathological assessment was made from paraffin-preserved samples. Casts were treated with phosphate-buffered saline (PBS) or tPA. Cast response to tPA was assessed by changes in cast weight and the production of fibrin D-dimer. Independent of dose, tPA reduced cast weight compared with PBS-treatment (P = 0.001) and increased D-dimer levels. Histological staining showed that PB casts from all patients were composed of fibrin and contained notable numbers of lymphocytes. Cast composition did not change over time. Collectively, these data support that in our PB patients, casts are composed of fibrin and are responsive to tPA treatment. This makes inhaled tPA a potentially viable option for symptomatic relief of PB while we work to unravel the complexity of PB pathogenesis.
Figures





References
-
- Barber BJ, Burch GH, Tripple D, Balaji S. Resolution of plastic bronchitis with atrial pacing in a patient with fontan physiology. Pediatric cardiology. 2004;25:73–76. - PubMed
-
- Brogan TV, Finn LS, Pyskaty DJ, Jr, Redding GJ, Ricker D, Inglis A, Gibson RL. Plastic bronchitis in children: a case series and review of the medical literature. Pediatr Pulmonol. 2002;34:482–487. - PubMed
-
- Buk SJ. Simultaneous demonstration of connective tissue elastica and fibrin by a combined Verhoeff's elastic-Martius-scarlet-blue trichrome stain. Stain technology. 1984;59:1–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
