

Further increases in carbapenem-, amikacin-, and fluoroquinolone-resistant isolates of Acinetobacter spp. and P. aeruginosa in Korea: KONSAR study 2009
- PMID: 21786445
- PMCID: PMC3159946
- DOI: 10.3349/ymj.2011.52.5.793
Further increases in carbapenem-, amikacin-, and fluoroquinolone-resistant isolates of Acinetobacter spp. and P. aeruginosa in Korea: KONSAR study 2009
Abstract
Purpose: The increasing prevalence of antimicrobial resistant bacteria has become a serious worldwide problem. The aim of this study was to analyze antimicrobial resistance data generated in 2009 by hospitals and commercial laboratories participating in the Korean Nationwide Surveillance of Antimicrobial Resistance program.
Materials and methods: Susceptibility data were collected from 24 hospitals and two commercial laboratories. In the analysis, resistance did not include intermediate susceptibility. Duplicate isolates were excluded from the analysis of hospital isolates, but not from the commercial laboratory isolates.
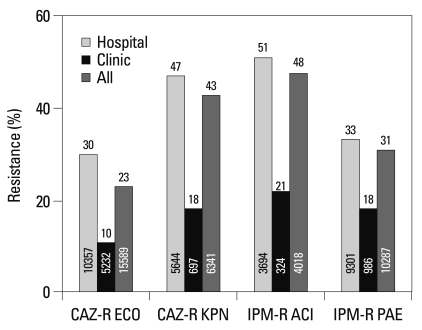
Results: Among the hospital isolates, methicillin-resistant Staphylococcus aureus, penicillin G-nonsusceptible Streptococcus pneumoniae based on meningitis breakpoint, and ampicillin- resistant Enterococcus faecium remained highly prevalent. The proportion of vancomycin-resistant E. faecium gradually increased to 29%. Ceftazidime-resistant Escherichia coli and Klebsiella pneumoniae increased to 17% and 33%, respectively, and fluoroquinolone-resistant K. pneumoniae, Acinetobacter spp. and Pseudomonas aeruginosa increased to 33%, 67% and 39%, respectively. Amikacin-resistant Acinetobacter spp. increased to 48%. Imipenem-resistant Acinetobacter spp. and P. aeruginosa increased to 51% and 26%, respectively. Higher resistance rates were observed in intensive care unit (ICU) isolates than in non-ICU isolates among the isolates from hospitals. Resistance rates were higher in hospital isolates than in clinic isolates among the isolates from commercial laboratories.
Conclusion: Among the hospital isolates, ceftazidime-resistant K. pneumoniae and fluoroquinolone- resistant K. pneumoniae, Acinetobacter spp., and P. aeruginosa further increased. The increase in imipenem resistance was slight in P. aeruginosa, but drastic in Acinetobacter spp. The problematic antimicrobial-organism combinations were much more prevalent among ICU isolates.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures





References
-
- Hsueh PR, Badal RE, Hawser SP, Hoban DJ, Bouchillon SK, Ni Y, et al. Epidemiology and antimicrobial susceptibility profiles of aerobic and facultative Gram-negative bacilli isolated from patients with intra-abdominal infections in the Asia-Pacific region: 2008 results from SMART (Study for Monitoring Antimicrobial Resistance Trends) Int J Antimicrob Agents. 2010;36:408–414. - PubMed
-
- Samuelsen O, Toleman MA, Sundsfjord A, Rydberg J, Leegaard TM, Walder M, et al. Molecular epidemiology of metallo-β-lactamase-producing Pseudomonas aeruginosa isolates from Norway and Sweden shows import of international clones and local clonal expansion. Antimicrob Agents Chemother. 2010;54:346–352. - PMC - PubMed
-
- Leclercq R, Derlot E, Duval J, Courvalin P. Plasmid-mediated resistance to vancomycin and teicoplanin in Enterococcus faecium. N Engl J Med. 1988;319:157–161. - PubMed
-
- Uttley AH, Collins CH, Naidoo J, George RC. Vancomycin-resistant enterococci. Lancet. 1988;1:57–58. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
