

Cytological results of ultrasound-guided fine-needle aspiration cytology for thyroid nodules: emphasis on correlation with sonographic findings
- PMID: 21786450
- PMCID: PMC3159940
- DOI: 10.3349/ymj.2011.52.5.838
Cytological results of ultrasound-guided fine-needle aspiration cytology for thyroid nodules: emphasis on correlation with sonographic findings
Abstract
Purpose: To compare the cytological results of ultrasound-guided fine-needle aspiration (US-FNA) cytology of thyroid nodules to sonographic findings and determine whether US findings are helpful in the interpretation of cytological results.
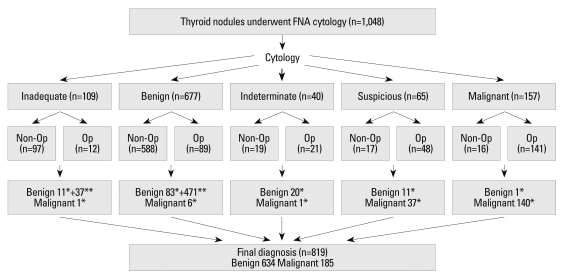
Materials and methods: Among the thyroid nodules that underwent US-FNA cytology, we included the 819 nodules which had a conclusive diagnosis. Final diagnosis was based on pathology from surgery, repeated FNA cytology or follow-up of more than one year. Cytological results were divided into five groups: benign, indeterminate (follicular or Hurthle cell neoplasm), suspicious for malignancy, malignant, and inadequate. US findings were categorized as benign or suspicious. Cytological results and US categories were analyzed.
Results: Final diagnosis was concluded upon in 819 nodules based on pathology (n=311), repeated FNA cytology (n=204) and follow-up (n=304), of which 634 were benign and 185 were malignant. There were 560 benign nodules, 141 malignant nodules, 49 nodules with inadequate results, 21 with indeterminate results, and 48 that were suspicious for malignancy. The positive and negative predictive values of the US categories were 59.1% and 97.0%, and those of the cytological results were 93.7% and 98.9%. The US categories were significantly correlated with final diagnosis in the benign (p=0.014) and suspicious for malignancy (p<0.001) cytological result groups, but not in the inadequate and indeterminate cytological results groups. The false positive and negative rates of cytological results were 1.9% and 3.2%.
Conclusion: Sonographic findings can be useful when used alongside cytological results, especially in nodules with cytological results that are benign or suspicious for malignancy.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures


References
-
- Mazzaferri EL, de los Santos ET, Rofagha-Keyhani S. Solitary thyroid nodule: diagnosis and management. Med Clin North Am. 1988;72:1177–1211. - PubMed
-
- Gharib H, Goellner JR. Fine-needle aspiration biopsy of the thyroid: an appraisal. Ann Intern Med. 1993;118:282–289. - PubMed
-
- Kelly NP, Lim JC, DeJong S, Harmath C, Dudiak C, Wojcik EM. Specimen adequacy and diagnostic specificity of ultrasound-guided fine needle aspirations of nonpalpable thyroid nodules. Diagn Cytopathol. 2006;34:188–190. - PubMed
-
- Cesur M, Corapcioglu D, Bulut S, Gursoy A, Yilmaz AE, Erdogan N, et al. Comparison of palpation-guided fine-needle aspiration biopsy to ultrasound-guided fine-needle aspiration biopsy in the evaluation of thyroid nodules. Thyroid. 2006;16:555–561. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
